
Since ACOs arrived in 2012 courtesy of the Section 3022: Medicare shared savings program, under Title III, Subtitle A, Part 3 of the Affordable Care Act (ACA) as the ‘new, new thing’ layered into a complex healthcare ecosystem peppered with more or less successful public/private efforts to restrain healthcare inflation, promote greater patient/member access, provide seamless coordinated care at lower per capita costs with better documented quality (the triple aim), ACOs have booked modest, variable but increasingly scalable impact via sponsored hosts from institutional health systems to physician driven enterprises.
A Brief Timeline
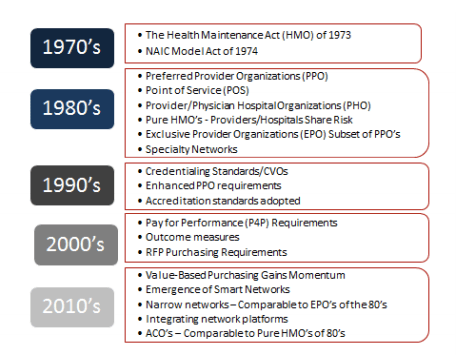
In 1973 President Richard Nixon signed into law the ‘HMO Act‘ officially launching ‘managed care‘ principally via closed ‘staff‘ and ‘group‘ model HMOs catering to niche (vs. ‘mainstream’) segments of key industry stakeholders, i.e., members (patients), employers, participating physicians and hospitals.
In the early to mid 80’s we witnessed the accelerated migration from narrow market penetration to mainstream medicine validation of the HMO model via the emergence of network models typically enabled by then emerging ‘Independent Practice Associations’ (IPAs).
Most IPAs emerged as a loose confederation of participating physicians as many physicians engaged out of a sense of curiosity or defensive hedging to not lose patients. First generation IPA’s featured at best tepid economic bonds, thus alignment of member physicians with the entity ‘leadership‘ (i.e., the Management Services Organization) goals were often ‘incidental considerations’ to many participating physicians. There just wasn’t enough ‘skin in the game‘ or economic integration, i.e., losing a withhold against a fee-for-service schedule just didn’t make that much of a difference from a total compensation point of view.
In the mid 80s principally in California Preferred Provider Organizations (PPOs) emerged and launched the era of discounted fee-for-services contracting for hospital, physician and ancillary services. PPOs were an HMO-lite version as members/beneficiaries voted with their feet within the network based on ‘in network’ benefit plan incentives vs. the closed loop (gatekeeper) HMO model.
In the 90s as mainstream initiatives continued to evolve and mature we witnessed the emergence of Physician/Hospital Organizations (PHOs) more often than not a joint venture between a host hospital (or parent health system) and a member physician organization (typically one or more IPAs or multi-specialty medical groups). PHOs were contracting vehicles and typically supported by an affiliate or owned MSO. Few PHOs entered into full risk arrangements with payors.
For prior comment and context on the evolving market, check out ‘Hey, Remember IPAs, PPOs and TPAs?’
Enter the ACO
While an ‘alphabet soup‘ of healthcare cost containment and quality improvement acronyms enshrined themselves into US healthcare delivery and financing lexicon (HMO, IPA, PPO, PHO, MSO, EPO, DPA, OWAs [other weird arrangements]), healthcare consumption of GDP continued it’s relentless upward growth – though somewhat moderated post passage of ACA.
In 2012 27 ACOs officially launched under the terms and provisions of the Medicare Shared Savings Program (MSSP) via a cohort sourced from 18 states serving an estimated 375,000 beneficiaries. Approximately half of the participating ACOs were physician-led, per the Center for Medicare and Medicaid Innovation (CMMI) – the administering agency.
Amidst ‘mixed results‘ considerable provider input to CMMI via open door forums and NPRM comments the ensuing years witnessed many tweaks to the rules associated with both the MSSP and Pioneer programs. In January of 2015 then Secretary of Health and Human Services Sylvia Burwell set goals for migration of payments from volume to valued based arrangements, see: ‘HHS Sets Specific Targets and Timelines for Alternative Payment Models and Value-Based Payment‘:
By the end of 2016, HHS plans to make 30 percent of FFS payments through APMs, such as accountable care organizations (ACOs) and bundled payments, and tie 85 percent of all FFS payments to quality or value. By the end of 2018, HHS intends to pay 50 percent of FFS payments through APMs, and tie 90 percent of FFS payments to quality or value.
This represents the first time in my 30+ years in healthcare delivery and financing innovation space that the Federal government has explicitly benchmarked industry migration away from its prevailing fee for services DNA.
While many pronounced ACOs as ‘DOA’ (dead on arrival) for many reasons, truth be told they’ve found their way into the managed competition ecosystem and are not going away anytime soon. In fact as is the case with most innovation, the ACO formula has been tweaked both in terms of its Government DNA (MSSP, Pioneer models, etc), and it’s private pay or commercial derivatives.
Meet the ‘Next Generation ACO Model’
The de facto amalgam of much of the lessons learned and serial tweaks imposed since the first class of ACOs launched in 2012 can be found in the Next Generation ACO Model, see: ‘The Next Generation ACO: Accelerating the Transformation from Volume to Value‘.
Per CMS, the model is defined as:
The Next Generation ACO Model is an initiative for ACOs that are experienced in coordinating care for populations of patients. It will allow these provider groups to assume higher levels of financial risk and reward than are available under the current Pioneer Model and Shared Savings Program (MSSP). The goal of the Model is to test whether strong financial incentives for ACOs, coupled with tools to support better patient engagement and care management, can improve health outcomes and lower expenditures for Original Medicare fee-for-service (FFS) beneficiaries.
Included in the Next Generation ACO Model are strong patient protections to ensure that patients have access to and receive high-quality care. Like other Medicare ACO initiatives, this Model will be evaluated on its ability to deliver better care for individuals, better health for populations, and lower growth in expenditures. This is in accordance with the Department of Health and Human Services’ “Better, Smarter, Healthier” approach to improving our nation’s health care and setting clear, measurable goals and a timeline to move the Medicare program — and the health care system at large — toward paying providers based on the quality rather than the quantity of care they provide to patients. In addition, CMS will publicly report the performance of the Next Generation Pioneer ACOs on quality metrics, including patient experience ratings, on its website.
A thorough application vetting process by CMS will assure participating ACOs admitted to the ‘NextGen’ cohort will present with the track record and capabilities to assume and manage the risk inherent in the model. Rather than bolt a new model on a legacy fee-for-services platform, CMS is fueling the necessary innovation to achieve the triple aim via a network of risk savvy ACOs.
Next Generations ACOs will deploy three (3) powerful ‘benefit enhancement‘ tools as they re-engineer clinical workflows and the prudent utilization of acute and sub-acute healthcare resources. This includes:
- Telehealth Expansion Waiver
- Post-Discharge Home Visit Waiver, and
- Three-Day Skilled Nursing Facility Waiver
 Featuring the ‘NextGen’ ACO Cohort
Featuring the ‘NextGen’ ACO Cohort
First up as we cycle through and profile best in class Next Generation ACOs is National ACO, led by industry pioneers and co-founders Andre Berger, MD, CEO and Alex Foxman, MD, FACP, President and Chief Medical Officer who serve as co-hosts of this series.
The series launches May 23, 2017 from 5PM – 5:30 PM Pacific/8PM – 8:30 PM Eastern. You can listen both live or on demand via This Week in Accountable Care.
We’ll discuss the model, their backgrounds and history in managed care and why they were drawn to form National ACO. We’ll close with comments from Alex Fair, CEO of the equity crowd funding platform Medstartr who will detail the recent listing of National ACO.
Join us!
==##==
*Editor’s Note: This post including This Week in Accountable Care broadcasts, periodic tweetchats via #ACOchat and blog posts in this series) are sponsored by National ACO, a Next Generation ACO. For more information on National ACO, click here.

Leave a comment