Editor’s Note: This is the first in a series of posts on ‘Patient Safety’ and specifically the NMP (“not my patient, not my problem”) problem in medicine.
I recently participated in the World Patient Safety Dayin Washington, D.C., September 17th, 2024, with organizing founding members of the Patients for Patient Safety, U.S., an affiliate of WHO (World Health Organization). We marched, then gathered for a ‘remembrance ceremony‘ for those lost, harmed or disabled due to medical error(s).
Anthony John Masters
The event is introduced by Martin J Hatlie, JD, President & CEO, Project Patient Care for Patients for Patient Safety Day D.C.:
The first post sets context for the series framing the nature of the problem and range of suggested solutions. Additional context for the series can be found at EndNMP.org
In 2016, a controversial study published in the British Medical Journal (BMJ) “Medical error—the third leading cause of death in the US” suggested that medical errors were the third leading cause of death in the United States, claiming over 250,000 lives annually. This statistic sent shockwaves through the medical community and sparked intense debate about both the accuracy of the number and the methodologies used to arrive at such estimates. Seven years later, we’re still grappling with the fundamental question: How many Americans actually die from medical errors each year?
The Current Landscape
Truth be told, we don’t know the exact number of deaths attributable to medical error(s) – and that’s part of the problem. Current estimates vary widely, ranging from 22,000 to over 440,000 (and above) deaths annually, reflecting the significant challenges in measurement and classification. The Centers for Disease Control and Prevention (CDC) doesn’t require reporting of medical errors on death certificates, and there’s no standardized methodology for capturing this data.
Why Such Wide Variations?
Several factors contribute to the dramatic range in estimates:
1. Definition Discrepancies: There’s no universal definitionof what constitutes a medical error. Some studies include only clear mistakes, while others encompass broader categories of preventable harm.
2. Reporting Mechanisms: Death certificates, the primary source for mortality statistics, don’t have a standardized way to indicate medical error as a cause of death.
3. Detection Challenges: Many errors go unnoticed or are not documented due to fear of litigation or professional repercussions.
Current Methodologies and Their Limitations
1. Global Trigger Tool (GTT) – Is a methodology developed by the Institute for Healthcare Improvement (IHI) to identify adverse events in medical records. It uses “triggers” (or clues) to identify possible adverse events, which are then investigated further to determine if an actual adverse event occurred.
Pros:
– Systematic approach using specific criteria
– Can identify errors that might otherwise go unnoticed
Cons:
– Labor-intensive and time-consuming
– Subject to reviewer interpretation
– May not capture all types of errors
2. Voluntary Reporting Systems
Pros:
– Can provide detailed information about specific incidents
– Helps identify patterns and systemic issues
Cons:
– Severe underreporting due to voluntary nature
– Bias towards more obvious or serious errors
3. Retrospective Chart Review
Pros:
– Comprehensive examination of patient records
– Can identify patterns and contributing factors
Cons:
– Time-consuming and expensive
– Subject to hindsight bias
– Limited by quality of documentation
The Case for Accurate Measurement
Despite definitional, measurement and reporting challenges, there are compelling reasons to pursue more accurate measurement of deaths from medical errors:
1. Patient Safety Improvement: Accurate data can help identify patterns and systemic issues, leading to targeted interventions and improved safety protocols.
2. Resource Allocation: Better data can inform where to focus quality improvement efforts and resources.
3. Accountability: Accurate measurement can drive accountability and motivate healthcare organizations to prioritize safety.
The Counterargument
Some argue that focusing too heavily on exact numbers could be counterproductive:
1. Defensive Medicine: Fear of being labeled as ‘error-prone‘ might lead to overly cautious medical practices and only reinforce what some referred to as the ‘blue wall of silence’, ie,, ‘thou shall not speak ill of one’s peers’.
2. Morale Impact: Constant focus on errors could demoralize healthcare workers and impact recruitment. ‘Clinical burnout‘ is already an epidemic for our often over worked and under supported clinicians.
3. Resource Diversion: Time and resources spent on measurement might be better used for direct patient care improvements and learnings from review of suboptimal outcomes, care gaps or poor handoffs during shift changes, etc.
Potential Solutions
Short-term Improvements
1. Standardized Definitions: Develop and implement consistent definitions of medical errors across healthcare systems.
2. Enhanced Reporting Systems: Create protected, anonymous reporting systems to encourage more accurate documentation.
3. Death Certificate Reform: Add specific fields for recording medical errors as contributing factors to death.
Long-term Strategies
1. AI and Machine Learning: Develop sophisticated algorithms to detect potential errors in real-time and analyze patterns across large datasets.
2. Culture Change: Foster an environment where error reporting is seen as a learning opportunity rather than a punitive measure.
3. National Database: Create a standardized, national system for recording and analyzing medical errors.
The Role of Technology
Emerging technologies offer promising solutions for more accurate measurement:
1. Natural Language Processing: Can analyze medical records to identify potential errors that human reviewers might miss.
2. Blockchain: Could provide secure, immutable records of medical events, making it easier to track and analyze errors.
3. Big Data Analytics: Can identify patterns and risk factors across large populations, potentially predicting and preventing errors before they occur.
Conclusion
While perfect measurement of deaths from medical errors may be an unrealistic goal, significant improvements are both possible and necessary. The path forward likely involves a combination of technological solutions, policy changes, and cultural shifts in the medical community.
As we work towards better measurement, we must balance the need for accuracy with the potential negative impacts of excessive focus on errors. The ultimate goal should be to create a healthcare system where errors are promptly identified, openly discussed, and systematically addressed – not to assign blame, but to save lives.
By taking a thoughtful, balanced approach to this challenge, we can work towards a healthcare system that is both more accountable and more effective at preventing harmful errors.
—
*Note to readers: This blog post aims to provide a balanced overview of a complex issue. The statistics and methodologies discussed are based on currently available research, but given the nature of the topic, exact numbers remain subject to debate and ongoing study.*
Whoa! Not 24 hours after the Request for Information (RFI) issued by WalMart Health and Wellness directed to it’s ‘strategic partner’ downline hit the street, I mean was leaked to the press, WalMart’s senior management felt compelled to promptly backdown from it’s rational, comprehensive, timely and sensible approach to make a meaningful dent into the US Healthcare, I mean, ‘Sickcare’ quagmire, by issuing the following terse statement:
Walmart Statement in Response to Health & Wellness Request for Information
“The RFI statement of intent is overwritten and incorrect. We are not building a national, integrated, low-cost primary care health care platform.”
– John Agwunobi M.D., Senior Vice President & President of Walmart U.S. Health & Wellness
Yikes! What’s behind this ‘whiplash’ effect?
It’s not news that WalMart has a mixed history with respect to the way they manage or evade (depending on your point of view) offering health benefits as an incentive to their less than full time staff. Yet, WalMart is the ‘400 pound gorilla’ as Chukwuma I. Onyeije, M.D., aka@chukwumaonyeije opined in a Google+ thread to a pool of health care social media peeps on Wednesday.
Regardless of the creative health benefits offer or ‘avoidance strategy’ for their part time staff, WalMart who’s gross sales account for approximately .5% of total US GDP, is a behemoth and perhaps second only to the Federal Government, the single largest ‘wholesale buyer’ of health benefits in the US.
So when they retained Price Waterhouse Coopers to consult on the compiling and distribution of an RFI to the tighly held ‘strategic partner’ network, they clearly intended to step into the population management fray of the payor/provider conundrum. You know, your costs are my revenues…
I’ve suspected all along, that while many on the provider side whine about CMS, the PPACA and now final rule to implement ACOs, many forward thinking peeps, mostly the Wall Street crowd who smell profits in those emerging re-engineered rules around population health management are stepping foward, perhaps aided and abetted by the so called ‘2nd in position skin in the game’ employer community.
We’ll watch and report with interest how this drama and retraction plays out.
How the Insurance Companies Took Over the HMO Industry & the Raid on FHP International
An Enhanced Reconstruction of the Robert Gumbiner MonographCross-referenced and augmented from oral history, SEC filings, corporate histories, and contemporaneous press sources
by Gregg Anthony Masters, MPH** Managing Director, Health Innovation Media | Executive Producer, Healthcare NOW Radio
Let me be direct: every policy conversation I’m having right now about ACOs, value-based care, and the so-called ‘transformation’ of American healthcare runs through a ghost – a Southern California physician who built something remarkable, watched it get strip-mined by a board and an investment banking culture that never understood what he’d built, and spent his final years putting the story on paper so we couldn’t pretend it didn’t happen.
His name was Robert Gumbiner, MD. His creation was FHP International Corporation. And his posthumously published monograph – The HMO, Taking It All Apart: The End of a Dream (AuthorHouse, 2009) is one of the most important and least-read documents in the history of American managed care.
I’ve been a soldier in this space long enough to have watched the managed competition experiment arc from insurgent idea to institutional furniture to convenient villain. I mainstreamed HMOs and second-generation PPOs in California back when the AMA still treated prepaid group practice like a communicable disease. So when I say Gumbiner’s story is our story – the story of everyone who has ever believed that organized, prevention-focused, physician-led care could actually work – I’m not being romantic. I’m being precise.
Before HMO Was a Dirty Word
Long Beach, California. 1961.
Gumbiner had already run the arc that defined his generation’s most serious physician-thinkers: Indiana University MD (1948), migration west, a stint as an Air Force physician during Korea, which exposed him to the logic of population-based capitated care and then a decade in private practice at Plaza Medical Group with nine other physicians, during which he’d been quietly running a prepaid plan for their patients. He understood, at an almost molecular level, what fee-for-service medicine was doing to the doctor-patient relationship: it rewarded illness, not health. He called it “basically immoral,” because it meant doctors earn the most when patients are sickest.
So in 1961, he converted Plaza Medical Group into a nonprofit corporation, Family Health Program, with 2,000 enrolled members prepaying a flat monthly fee for comprehensive care delivered by employed physicians under one roof. This is what we now call the staff-model HMO. At the time, it was barely tolerated by organized medicine and invisible to most health policy observers.
By the end of the 1950s, Gumbiner recalled in the Orange County Business Journal, “there were only a few dozen HMOs around the country.” When he launched, the concept had a lineage, i.e., Kaiser’s industrial prepaid plans from the 1930s, the Group Health Association in DC, but it was emphatically not mainstream. It was, in fact, exactly the kind of structural insurgency (in today’s parlance ‘innovation’) that establishment, legacy or mainstream medicine and insurance industry incumbents were designed to suppress.
What Gumbiner built over the next two decades is, by any honest accounting, one of the great organizational achievements in American healthcare history:
1967: 10,000 members. Second Long Beach center.
1968: Third center, Fountain Valley, Orange County.
1969: Medicaid pilot launched, one of the first HMOs in the country to serve low-income beneficiaries, at a time when most of the industry thought Medicaid was financial poison.
1971: 30,000 members at the ten-year mark. Compton center added.
1973: Guam. Which tells you everything about his ambition and his eccentricity.
1977: Federal HMO qualification, opening eligibility for Medicare and Medicaid reimbursement.
1982: Medicare risk contract pioneer – Family Health received a federal demonstration contract to provide prepaid capitated care to seniors, assuming full actuarial risk that the patient’s care might exceed the flat fee. This is the model that became Medicare Advantage. Gumbiner’s shop essentially invented it for the West Coast.
1983: FHP Senior Plan launched. The company converted a Long Beach skating rink into a Senior Health Plan Center to handle the flood of new elderly members.
I’ve thought about that gap for a long time. At the time, it looked like savvy maneuvering. In retrospect and this is the argument Gumbiner makes explicitly in his monograph and in the two-volume oral history he gave to UC Berkeley’s Bancroft Library in 1996, it was the opening through which a different set of institutional logics entered the organization. The IPO followed in July 1986 on NASDAQ. The board composition changed. Wall Street’s quarterly cadence became a structural fact of life. And the incentive architecture that had produced three decades of mission-driven growth began, slowly, to be reoriented around something else entirely – something I’ve referred to as the ‘HealthcareBorg‘ where all meaningful innovation goes to die via assimilation by the incumbents – which just might explain the hostility towards the entire for profit health insurance domain.
The IPA expansion accelerated during this period via more mainstream docs in Individual Practice Associations, networks of independent physicians contracted rather than employed. Faster to stand up than a new medical center, cheaper in capital terms, easierto scale across new geographies. Also, in Gumbiner’s view, a vector through which fee-for-service logic seeped back into what was supposed to be a capitated, prevention-focused enterprise. You cannot supervise the clinical behavior of 10,000 contracted independent physicians the way you can manage 200 employed ones. The model that made FHP FHP, i.e., an integrated, accountable, coherent ecosystem, began to diffuse.
In 1990, Gumbiner stepped back from day-to-day operations. The board was now running the company. Within months: a major malpractice jury award. A Medicare rate increase of only 1.4 percent. Federal scrutiny of FHP’s aggressive Medicare marketing in San Diego. The architecture was holding, but the foundation had shifted.
FHP at that moment served nearly 2 million HMO members in 11 states and Guam – commercial, governmental, and Medicare beneficiaries – across ambulatory care, hospital services, pharmacy, dental, vision, home health, skilled nursing, physical therapy, psychological counseling, and health education. The combined entity would serve almost 4 million members in 15 states with revenues exceeding $8.5 billion.
Consumer and physician groups urged state regulators to block it. The market concentration numbers were legitimately alarming:47 percent of the Medicare HMO market in Los Angeles County, 66 percent in Orange County, 70 percent in San Diego County. The California Medical Association opposed it on efficiency grounds, the evidence that large-company mergers produce meaningful savings was thin then and it’s still thin now. The FTC investigated. The state AG investigated. Neither acted. The merger closed in early 1997.
And Gumbiner, who had built this thing across 35 years, who had invented the Medicare risk contract, who had created clinical infrastructure across nine states when managed care was barely a concept, was out.
I’m writing this for ACO Watch, which means my readers understand the through-line I’m about to draw. So let me draw it directly.
The organizational model Gumbiner built, i.e., prepaid, prevention-focused, fully integrated, actuarially disciplined, with employed physicians and owned facilities, is what every serious accountable care framework since 2010 has been trying to reconstruct, imperfectly, at scale, inside a payment system that was never designed to support it. The MSSP. ACO REACH. The forthcoming LEAD Model. They are all, in their distinct ways, attempts to reimpose Gumbiner’s original logic onto a fee-for-service chassis that keeps metabolizing the intervention and returning to equilibrium, ergo the assimilation phenomenon.
The fundamental misalignment he identified, i.e., a payment system that rewards illness management over health maintenance, has not been solved. It has been managed around, at the margins, with shared savings arrangements that generate meaningful but modest results. MSSP produced a record $2.4 billion in savings in 2024, and that’s real. It’s also modest relative to total Medicare spend, and the structural incentive failure underneath it is still compounding.
What Gumbiner’s story adds to that conversation is a specific and underappreciated caution: governance matters as much as model design. FHP didn’t fail because prepaid group practice was wrong. It was absorbed (assimilated then corrupted) because the governance structure, i.e., the board composition, the shareholder dynamics, the CEO succession, drifted away from the founding logic without anyone being able to stop it. The mission got managed out of the mission-driven organization.
So as Sachin Jain recently opined, it’s about leadership. Nope! It’s the ‘OG&E’ (organization. governance and equity) foundation. Every ACO, every value-based care arrangement, every innovative primary care model operating inside a larger health system is subject to exactly this risk. The same board dynamics, the same quarterly earnings pressure, the same management consulting ‘Beltway Bandit‘ logic, i.e., B Cubed where bullshit baffles brilliance, almost reflexively says consolidation creates efficiency, yada, yada, yah. These are the forces that ended FHP, and they are operating today with considerably more sophistication and regrettably due to our healthcare ‘leaders‘ failure to lead, with considerably less resistance or pushback.
The Third Career, and What It Tells Us
There’s a postscript to the Gumbiner story that I find both moving and instructive.
After FHP was absorbed in 1997, Gumbiner turned to a project he’d been incubating since his first trip to Latin America in the early 1960s: the Museum of Latin American Art (MOLAA) in Long Beach, the only museum in the United States dedicated exclusively to modern and contemporary Latin American and Latino art. He purchased a former skating rink (a building type he apparently had a gift for repurposing), connected it to a former silent-movie studio, and spent more than $40 million over a decade building something remarkable. At his death in January 2009, he bequeathed over $50 million to MOLAA and the Robert Gumbiner Foundation.
He also funded the Ethnic Art Institute of Micronesia on the island of Yap. Of course he did.
Here’s what I take from the third career: Gumbiner was constitutionally a builder. He built 55 medical centers and four hospitals in nine states in his second career and then turned around and built a world-class art museum in his third. What he could not build, in the end, was an institutional structure durable enough to outlast the forces that came for it once the company went public and the governance shifted.
That is the cautionary lesson that belongs in every conversation about ACO governance, value-based model sustainability, and what happens to mission-driven organizations when they intersect with capital markets.
The dream was right. The architecture was real. The board got captured. And a $2.1 billion transaction later, it was over. Sound familiar (think the current dangerous to global and U.S> public health Charlatan at HHS and his unfit to lead minions at the commanding heights of our public health infrastructure.
The HMO, Taking It All Apart is available through Internet Archive and worth every hour it takes to read. Gumbiner earned the right to be bitter. He chose, instead, to be specific and to leave the record straight.
We should be paying attention.
==##==
** ** AI Use & Editorial Standards Disclosure. In producing this content, the author employed AI language tools in a defined supporting role: (1) Research aggregation: surfacing relevant source material and authoritative references across peer-reviewed, institutional, the arts and journalistic databases; (2) Structural organization: proposing content architecture and draft sequencing; (3) Draft suggestion: generating candidate language for author review. The author retains sole editorial responsibility for all published content. Every citation is independently confirmed as accurate and accessible prior to publication. No headlines, pull quotes, or factual claims are published without author verification. AI-generated language is treated as raw material then recast entirely in the author’s established voice and subject-matter expertise before any content reaches publication. This workflow reflects the author’s commitment to the standard that AI serve, not replace the author.
Part I: Leadership Isn’t the Problem. Leadership Is the Symptom.
By Gregg Anthony Masters, MPH**
Today I read a piece quoting the insights of Sachin H. Jain, MD, MBA, FACP, CEO of SCAN Group, SCAN Health Plan, and Forbes contributor, titled: “Healthcare’s problem isn’t the system, it’s us”.
The core argument:
The “it’s us“ indictment. In each of his three decades in healthcare, Jain has faced a different “boogeyman,” from the quality crisis to coverage expansion to today’s push toward value-based care. Each time, the industry implemented a fix, yet nothing improved. His conclusion: “It’s us. We’re not necessarily taking charge of the problems that are under our control.”
Toxic positivity as strategic evasion. Rather than acknowledging the real anger over cost, denials, and administrative burden, executives simply pointed to the flawed system. Jain’s view: “You can’t fix something until you actually acknowledge it’s a problem.” He concluded bluntly: “No one’s buying it anymore.”
The “no margin, no mission” trap. Jain cited a cardiologist at a Northeast academic medical center who built a heart failure program keeping patients out of the hospital. The hospital’s response was to ask what the department was doing wrong since admissions had dropped. When the physician explained the program was working, he was told: “No margin, no mission.” Jain argued this phrase has become a cover for exactly the kind of leadership failure he was describing.
Latent leadership capacity being killed. “We have so much more latent leadership capacity in this industry than we’re exercising. We have so many people with so much ingenuity, creativity, drive and passion, and we kill it.” His prescription: the number one way to improve healthcare is to tap leaders who genuinely support and desire an improved system.
Courageous challenge as organizational culture. At SCAN, Jain has made “courageous challenge” a core organizational value, giving employees explicit permission to stand up and say something that goes against the grain, creating an environment where difficult conversations and hard questions are not just tolerated but encouraged.
Accountability means being reachable. Every quarter, Jain sends his personal work email to each of SCAN’s 440,000 members and reads three types of messages daily: one from a satisfied member, one offering helpful advice, one who is angry. His view: “We hide behind HIPAA, we hide behind the ACA, we hide behind whatever rules we think we can hide behind.” vaticahealth
Depth over breadth, “monogamy” in provider-plan relationships. Jain argued healthcare is “extraordinarily promiscuous,” with providers partnering with every plan and plans partnering with every provider group. No one builds anything deep enough to change the patient experience. He pointed to SCAN’s strategy of asking provider partners to stop splitting membership across every plan and work with SCAN exclusively, asking what it would look like to have a shared call center, a shared patient record, and shared accountability for outcomes.
This ‘fireside chat’ triggered and prompted reflection on his argument and the need to reply via a series of posts to this audience.
Every generation of healthcare executives believes it has inherited a uniquely broken system.
It hasn’t.
American healthcare has been declared “unsustainable” almost continuously since Medicare and Medicaid were enacted in 1965. Costs have risen. Technology has advanced. Institutions have consolidated. Payment models have evolved from indemnity insurance to HMOs, PPOs, ACOs, bundled payments, Medicare Advantage, Direct Contracting, ACO REACH, and now artificial intelligence-enabled utilization management.
Yet one uncomfortable fact remains. The underlying economics have changed remarkably little.
That is why Sachin Jain’s recent essay, Healthcare’s Problem Isn’t the System – It’s Us, deserves attention. His central argument is provocative precisely because it rejects one of healthcare’s favorite excuses, i.e., that “the system” (aka the @HealthcareBorg) is somehow responsible for our collective inability to transform care and optimize outcomes.
He argues instead that healthcare’s greatest obstacle is leadership. Executives normalize dysfunction, defer difficult decisions, and hide behind complexity instead of exercising moral courage. It is a compelling critique because it contains more than a grain of truth.
Indeed, leadership matters. Organizations do not transform themselves. People do. But I would suggest Jain’s diagnosis stops one layer too soon:
Leadership is not the disease.
Leadership (or some may say absence of) is the symptom.
The disease is an incentive structure that rewards institutional preservation over institutional transformation.
That distinction matters because it explains why otherwise capable leaders repeatedly make decisions that appear timid, contradictory, or strategically incoherent.
We Don’t Have a Leadership Crisis
Contrary to popular opinion, American healthcare does not suffer from a shortage of intelligent executives. Quite the opposite.
Healthcare is populated by extraordinarily talented physicians, administrators, economists, data scientists, entrepreneurs, operators and yes, even actuaries. Few industries possess comparable intellectual capital.
Nor is there a shortage of strategic plans. Every health system now speaks fluent “value.” Every payer proclaims patient-centeredness. Every annual report celebrates innovation. Every conference keynote extols digital transformation. Every strategic retreat promises to “meet patients where they are.”
And yet fee-for-service continues to dominate organizational behavior. Not because executives secretly oppose value-based care. Because they are compensated to preserve existing revenue streams while cautiously experimenting around the edges.
That isn’t cowardice. It’s governance.
Boards hire CEOs to protect enterprise value.
Bond ratings.
Operating margins.
Market share.
Debt covenants.
Credit access.
Political relationships.
Employment stability.
The healthcare CEO who voluntarily cannibalizes profitable fee-for-service revenue in pursuit of uncertain long-term value may be admired by academics. Yet, he or she is far less likely to survive the next compensation committee meeting.
Leadership, in other words, operates within constraints that are rarely acknowledged in popular discussions about healthcare transformation.
Culture Doesn’t Create Incentives
Healthcare management literature frequently asserts that “culture eats strategy for breakfast.” The aphorism has become management orthodoxy. But in healthcare, incentives generally eat culture. Yet, truth is ‘culture’ follows payment. One need only observe how quickly provider behavior changes when reimbursement changes:
Hospital admissions.
Observation status.
Readmission penalties.
Risk coding.
Quality reporting.
Telehealth.
Hospital-at-home.
Every one of these evolved not because organizational culture suddenly matured but because financial incentives shifted.
Executives responded rationally.
As they should. This is not a moral failure. It is economics, full stop. Healthcare organizations are adaptive organisms. They evolve toward reimbursement, often quoting ‘no margin, no mission’.
The Myth of “The System“
Ironically, I agree with Jain on one point. Healthcare leaders often invoke “the system” as though it were weather. Immutable. Uncontrollable. An external force beyond human agency. But systems are not acts of nature. They are collections of incentives designed and continually redesigned by policymakers, regulators, employers, insurers, providers, investors, and consumers. The system behaves exactly as it has been designed to behave. Its outcomes may be undesirable. They are rarely accidental.
The ‘Missing’ Conversation
What remains surprisingly absent from contemporary healthcare leadership discussions is political economy, i.e., you can’t implement policy absent the enabling politics of ‘winning’ elections. Healthcare does not merely allocate clinical resources. It allocates financial power (minimally think proceduralist vs cognitive biases). Every reform proposal creates winners and losers. Every payment redesign redistributes income. Every consolidation shifts bargaining leverage. Every new benefit changes market share. Leadership, to the extent it can be ‘homogenized’ into best practices, alone cannot overcome those structural realities. Nor should we expect it to.
A Generation of ‘Deferred’ Decisions
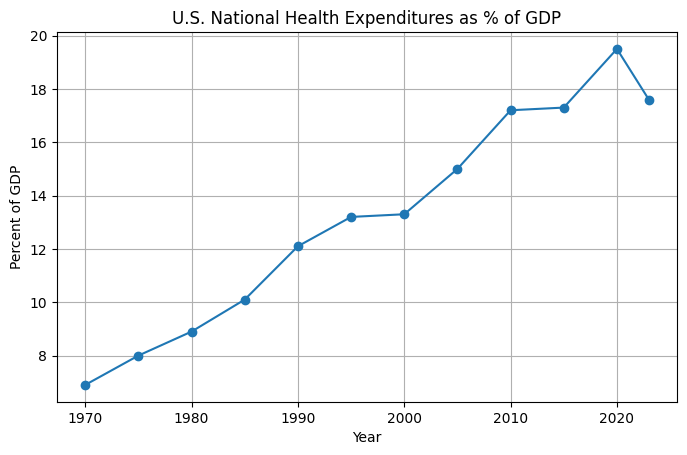
The irony is both persistent and painful. The healthcare industry has spent nearly forty years‘discussing’ transformation. When I started the GDP of healthcare share was 8-9 % range, today it’s just shy of 20%.
Secular themes, you know the organizing value proposition of push/pull industry top lines at major healthcare innovation conferences from HiMSS to HLTH with many in between including Health Datapalooza, JP Morgan Investor Healthcare Conference, NextMed (formerly Exponential Medicine and FutureMed, etc.) popularly engage:
Disease management.
Managed competition.
Integrated delivery.
Consumer-directed care.
Medical homes.
Population health.
Accountable Care Organizations.
Precision medicine.
Digital health.
Artificial intelligence.
Each promised structural change. Most produced incremental adaptation where one-off or niche (think Dave Chase and Rosetta innovation for self-funded employer sponsored health plans) vs. ‘systemic’ relief, i.e., advancing the triple let alone more ambitious ‘quadruple’ aim of clinician work/life satisfaction.
Why?
Because almost every reform was layered on a chassis of existing fee-for-service economics rather than replacing them. We reflexively create hybrid systems instead of new systems. Organizations therefore learned to optimize for both worlds simultaneously. Volume finances value. In turn value justified volume. Everyone learned the language and adopted the culture. Few changed the business model or associated incentive structure.
Where I Part Company with Sachin
This is where my conversation with Sachin begins rather than ends. He asks why leaders tolerate the status quo. I ask why boards reward them for doing so. He emphasizes courage. I emphasize incentives. He sees latent leadership. I see institutional equilibrium. Neither perspective is mutually exclusive. But one operates upstream from the other.
Coming Next
The debate over leadership inevitably leads to a larger historical question. How did American healthcare arrive here? Ironically, many of today’s strategic dilemmas were anticipated nearly forty years ago by one of managed care’s most consequential and controversial architects. Leonard D. Schaeffer believed healthcare organizations would eventually have to stop trying to partner with everyone. Instead, they would have to choose strategic allies capable of building scale together. Whether history vindicated that vision, or exposed its limits, is the subject of Part II.
==##==
Editor’s Note:
For Part II, I’ll trace Leonard Schaeffer’s move from HCFA to Blue Cross of California in 1986, the turnaround, the creation of WellPoint in the early 1990s, and the strategic logic behind selective payer-provider alignment, grounded in contemporaneous sources and Schaeffer’s own writings.
** AI Use & Editorial Standards Disclosure. In producing this content, the author employed AI language tools in a defined supporting role: (1) Research aggregation: surfacing relevant source material and authoritative references across peer-reviewed, institutional, the arts and journalistic databases; (2) Structural organization: proposing content architecture and draft sequencing; (3) Draft suggestion: generating candidate language for author review. The author retains sole editorial responsibility for all published content. Every citation is independently confirmed as accurate and accessible prior to publication. No headlines, pull quotes, or factual claims are published without author verification. AI-generated language is treated as raw material then recast entirely in the author’s established voice and subject-matter expertise before any content reaches publication. This workflow reflects the author’s commitment to the standard that AI serve, not replace the author.
by Gregg Anthony Masters, MPH & Fred Goldstein, MS **
PopHealth Week | Healthcare NOW RadioHost: Fred Goldstein, President, Accountable Health, LLC Executive Producer & Co-Host: Gregg Anthony Masters, MPH Episode Theme: “Enough Is Enough” – The Decimation of Public Health Infrastructure, the Rise of Health Quackery, and Why Science Still Matters
“Silence is acceptance people. Speak up!” – Gregg Anthony Masters, MPH, closing the episode
Introduction: When Professionals Say Enough
There comes a moment, sometimes quiet, sometimes explosive, when a person who has spent decades navigating institutions, absorbing dysfunction of ‘managing’ complex enterprises whether health plans or health systems, and advocating for incremental reform simply decides: no more. That moment arrived for Fred Goldstein, President of Accountable Health, LLC, and a recognized voice in population health, managed care, and evidence-based healthcare delivery.
On this episode of PopHealth Week, Fred once again stepped into the guest SME (subject matter expert) chair to unpack the essays he published on his PopHealth Pulse and LinkedIn under a title that said everything: “Enough is enough” and “People, Health, Research and Reality”.
His executive producer and co-host for the day, Gregg Anthony Masters, MPH, framed the conversation squarely and without ceremony: this was about the systematic dismantling of public health infrastructure, the ‘weapon-ization’ of social media against scientific literacy, and the long-unresolved contradiction at the heart of American healthcare – a system that was never really designed to produce health.
What followed was one of the most direct, experience-grounded conversations in the show’s run. No hedging. No false balance. Just two seasoned public health professionals, credentialed and candid, saying what the data and their careers have confirmed.
Part I: What “Public Health Infrastructure” Actually Means
One of Gregg’s most clarifying moves was to refuse the narrow definition of public healthinfrastructure and insist on the broader one. In popular discourse, “public health” often conjures health departments, ie, chronically underfunded agencies staffed by mission-driven clinicians who, as he put it, had to be “heart centered” to choose that career path “because the money ain’t there.”
But Fred and Gregg broadened the frame deliberately: legacy public health infrastructure (underfunded, often understaffed, overworked health departments, poorly synced with acute health care assets – think the ineffective handoff of Ebola cases in Dallas circa 2014) includes CMS, Medicare, Medicaid, and the full architecture of Title (XIX & XX) programs that fund and structure American healthcare delivery. It includes the research enterprise at NIH and the critical international disease surveillance network anchored by USAID. It includes housing policy, clean water, education, and the social determinants of health that account, by most estimates, for 80 percent or more of health outcomes.
This is not a rhetorical expansion. It is epidemiologically accurate. The World Health Organization defines social determinants of health (WHO) as the conditions in which people are born, grow, live, work, and age, coupled with decades of research confirm that income, housing stability, educational attainment, and neighborhood safety drive health outcomes more powerfully than any clinical intervention. When you defund housing programs, you are defunding health. When you eliminate food assistance, you are eliminating a health intervention. The infrastructure is one system, even if it is administered across dozens of agencies.
Fred named the pattern plainly: “what is being cut is not bureaucratic waste. It is the scaffolding that keeps people alive.”
Part II: DOGE, USAID, and the Epidemiological Consequences of Dismantling Global Surveillance
The conversation turned to one of the most consequential policy decisions in recent memory: the near-total dismantling of the United States Agency for International Development (USAID). Fred and Gregg cited this as one of the worst offenses in the broader campaign of senseless institutional destruction of modest public health interventions with a very high ‘return’ to the community.
USAID’s public health programs were not primarily charity. They were strategic. The agency maintained disease surveillance networks across dozens of countries, funded outbreak response capacity, and supported the kind of early-warning infrastructure that gives health systems time to respond before a pathogen becomes a pandemic. PEPFAR, administered through USAID, has saved an estimated 26 million lives since its 2003 launch. USAID’s tuberculosis programs treat millions annually in countries where, without treatment, extensively drug-resistant strains develop and spread – including, eventually, to the United States.
Fred stated the logic simply: we are interconnected. Pathogens do not respect borders or visa requirements. “Someone comes across on a cruise or a boat,” he said or, as the COVID-19 pandemic demonstrated, on a plane connecting through a major international hub. The current Ebola outbreak in the Democratic Republic of Congo was offered as a live example: the same kind of outbreak USAID was built to monitor and contain at the source.
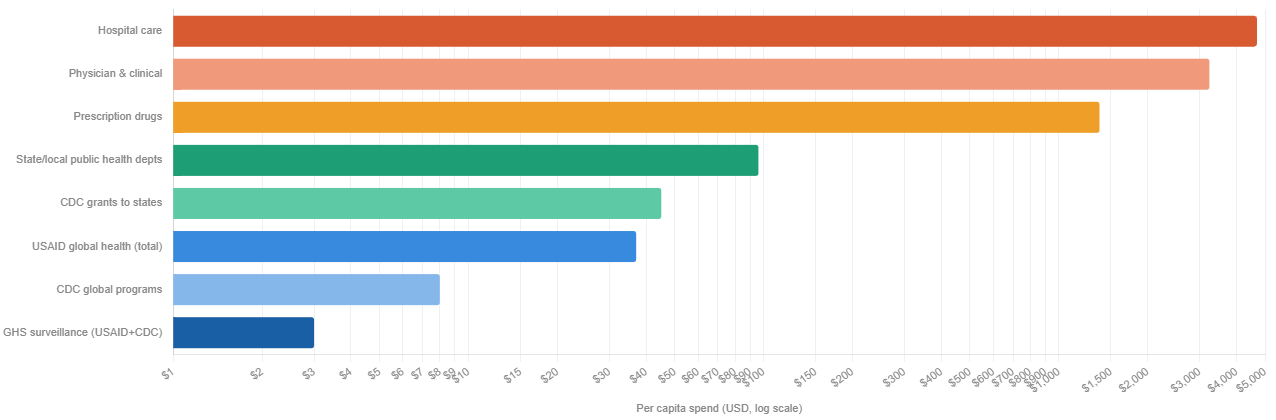
Investments in disease management vs. public health infrastructure
Ratio: hospital care vs. global surveillance 565:1
per dollar spent on global health security (GHS) programs
Public health as share of total spend
all prevention combined, per TFAH
COVID economic cost vs. 5-yr GHS spend
$14T loss vs. $1B prevention investment
Sources: CMS National Health Expenditure Accounts 2024; KFF; Trust for America’s Health; GAO; Johns Hopkins Center for Health Security. US population ~335M used for per capita calculations. CDC global programs ~$700M; GHS combined USAID+CDC ~$993M (FY2025 CR level). State/local public health includes federal grants to states.
The Centers for Disease Control’s Global Disease Detection program, which partnered closely with USAID, exists precisely because the cost of surveillance is a fraction of the cost of pandemic response. A 2019 report by the Johns Hopkins Bloomberg School of Public Health estimated that a severe respiratory pandemic could cost the global economy $570 billion annually. Defunding the early-warning systems that prevent such events is not fiscal prudence. It is a catastrophic risk transfer from the present to the future.
Part III: NIH Cuts and the Strategic Suicide of Defunding Research
Fred’s frustration was palpable when the conversation turned to NIH funding cuts. “The idea of cutting these NIH funds around research is just bonkers,” he said. “This country has been amazingly great and built upon the power of research.”
This is not nostalgia. It is economics. The National Institutes of Health funds research that has produced more pharmaceutical breakthroughs, more diagnostic innovations, and more clinical protocols than any comparable institution on earth. A United for Medical Research (UMR) 2026 Report: “NIH’s Role in Sustaining the U.S. Economy FY 2025” analysis found that every federal dollar invested in NIH research generates roughly $2.57 in economic activity. The mRNA technology underlying COVID-19 vaccines, developed with substantial NIH funding over decades, saved millions of lives and demonstrated that basic research investment has compounding returns that are impossible to predict in advance but catastrophic to forgo.
Fred invoked the HIV/AIDS research arc as the definitive case study in scientific iteration. From the first clinical descriptions of a mysterious immunodeficiency syndrome in 1981 to the identification of HIV, the development of AZT, the breakthrough of triple-combination antiretroviral therapy, the elucidation of viral load and CD4 counts as clinical markers, and the current era of PrEP, which can reduce the risk of getting HIV acquisition risk by as much as 99 percent in those who take it consistently – the arc took four decades of funded, iterative, sometimes-wrong-but-self-correcting science. None of it would have happened without sustained public investment.
“You never know what’s going to come out of some research project,” Fred noted. “It may lead to another great discovery.” This is not a platitude. It is the documented history of penicillin, of the polio vaccine, of chemotherapy, of statins. Defunding research does not eliminate need. It eliminates the capacity to meet it.
Part IV: The Scientific Literacy Crisis – How We Got Here and Why It Matters
Perhaps the most sobering section of the conversation addressed why false health claims spread so much faster than evidence. Fred and Gregg identified a convergence of forces:
1.Education gaps around scientific process. Most Americans never learn what science actually is, an iterative, self-correcting methodology that moves, as Gregg put it, “from unreasonable certainty to reasonable uncertainty.” Science does not produce Truth with a capital “T” on first contact. It produces provisional, probability-weighted conclusions that grow stronger with replication. That is not a weakness. That is the mechanism. But to someone who has never been taught how science works, the iterative nature looks like inconsistency, and inconsistency looks like unreliability.
2.Abbreviated attention spans. Fred cited an observation from a film school that younger students are struggling to sit through feature-length films because short-form social media content has restructured their attention patterns. The American Psychological Association (APA)has documented the relationship between heavy social media use and reduced capacity for sustained attention. Short-form claims, delivered with confidence, are cognitively easier to process than qualified, data-heavy arguments. Misinformation is almost always shorter than the truth.
3. The amplification of confident wrong voices. Fred described listening to a social media personality with millions of followers making claims he found “completely crazy.” His sons listened for ‘entertainment’. Millions listened for ‘guidance’. The Reuters Institute Digital News Report has consistently found that significant portions of the public receive health and science information through social media, often from sources with no relevant credentials.
4. The supplement and wellness industry’s exploitation of regulatory gaps. The Dietary Supplement Health and Education Act of 1994 created a framework in which supplement manufacturers bear no pre-market burden to demonstrate efficacy or safety. Claims that products “support” various functions proliferate without double-blind trials. Fred identified this as a deliberate exploitation of public scientific illiteracy and named it accurately as ‘health quackery’, given new life by a policy environment that values bold declarations over peer review.
Part V: The ADA Conference Incident – When Institutions Suppress Dissent
One of the episode’s most striking moments came when Fred described a scene at the American Diabetes Association’s recent scientific conference: researchers who had published an editorial in the ADA’s own journal, concerning NIH cuts and research funding, were handing out copies of that published work at the conference. They were escorted out by police!
This deserves to sit with you for a moment. A peer-reviewed article. In the associations own journal. Distributed at the association’s own conference. And the authors were removed by law enforcement.
Fred noted that subsequent resignations from the ADA followed. Gregg named the dynamic without euphemism: “there is a chill”. Professional associations that depend on relationships with federal funders, on conference sponsorships, and on not provoking regulatory scrutiny are making institutional calculations that silence their own members.
This is not unprecedented. Research on self-censorship in scientific communities has documented the ways in which funding dependencies, career pressures, and fear of political backlash suppress scientific speech, particularly on contested policy questions. What is notable is how openly it is now happening, and how quickly institutions that existed to advance scientific knowledge are retreating from that mission when it becomes inconvenient.
Part VI: The Broken Healthcare System: A Disease That Predates DOGE
Both Fred and Gregg were careful to separate two problems that are related but distinct:
Problem One: The current administration’s cuts to research, public health infrastructure, and social support programs. This is acute damage being done in real time.
Problem Two: The structural failure of the American healthcare delivery and financing system. This is chronic. It predates the current political moment by decades.
Gregg has tracked the evolution of this system with the granular attention of someone who has lived inside it. He walked through the arc: HMOs, then IPA spin-offs, followed by PPOs (which were more “palatable” to the group health market that didn’t want narrow networks), the ACA (Affordable Care Act) introduced ACOs, value-based care organizations, and corporate managed care organizations in various iterations. None of them, he noted, have solved the fundamental problem. They have created “more hurdles and obstacles for people to jump through to get needed care.”
Meanwhile: costs continue to accelerate driving widespread affordability claims as more and more of the liability shifts from plan to member via increased premiums, copays, coinsurance and deductibles due in large part due to the failure of House and Senate Republicans to extend ACA premium tax credits (subsidies). Meanwhile, access remains spotty. And quality is, in Gregg’s word, “a crapshoot.”
Gregg referenced a colleague’s new book “Healing the Sick Care System and Why Patients Matter” by Gil Bashe, which argues that the healthcare system views itself as the client, not patients. Fred agreed with the diagnosis but offered a defense of physicians: most clinicians entered medicine to help. The system does not allow them to. If a primary care physician in a fee-for-service environment keeps a patient healthy, that physician makes less money. A healthy patient generates no revenue. As Gregg further articulated: “There is no prevention business model as long as you run on a fee-for-service chassis.”
This is a structural incentive problem, not a character problem. And it is one that decades of health economics research has confirmed. Fee-for-service payment rewards volume and complexity. It penalizes efficiency and prevention. Value-based care models have attempted to reorient incentives, but Fred cited research suggesting the results have been modest at best – bending a 4 percent cost trend to 3.5 percent is not the systemic transformation advocates hoped for. The system, as he put it, “will not let” costs actually drop.
The brutal arithmetic of insurance: a health plan that successfully keeps its population healthy will collect premiums on a healthier pool, generate fewer claims, and in the ACA (Affordable Care Act) medical loss ratio framework find itself returning money if its loss ratio drops too low. The financial incentive structure does not reward health. It rewards the management of illness at a profitable margin.
Part VII: Physician Burnout as a System Failure, Not a Personal Failure
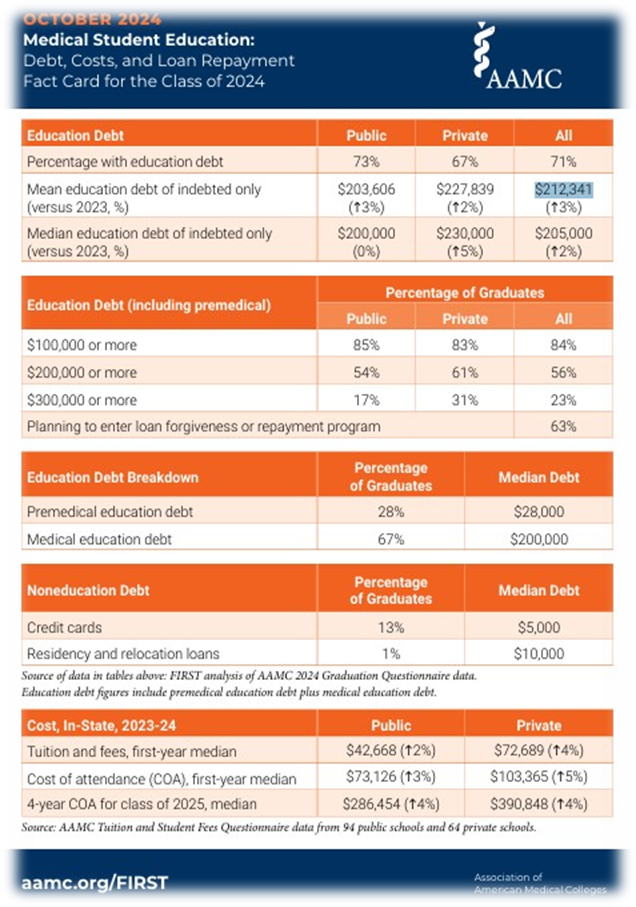
Gregg raised what he described as the ‘brain drain’ waste embedded in physician training coupled with growing exits to entrepreneurial or other administrative roles, ie, CMIOs. The public investment in producing a physician – four years of undergraduate education, four years of medical school, three to five years of residency, often additional fellowship training – represents up to a sixteen years of intensive investment, plus a debt load that for many physicians (public and private) averaged $212,341 according to Association of American Medical Colleges (AAMC) Medical Student Education: “Medical Student Education: Debt, Costs, and Loan Repayment Fact Card for the Class of 2024 “.
When those physicians burn out and exit clinical practice, opting for administrative roles, i.e., CMO (chief medical officer) and other positions, entrepreneurial ventures, or simply early retirement, the human capital loss is staggering.
The root cause is notindividual weakness. It is system design. Dr. Tait Shanafelt,professor of medicine and chief wellness officer at Stanford Medicine, describing the cultural mindset that long prevailed:
“There was this rite of passage mindset of: I went through it, it was formative – you should go through it too.”
Further, AMA research on physician burnout has documented the relationship between administrative burden, moral injury (being unable to provide care one knows is necessary), and the psychological costs of navigating prior authorization, documentation requirements, and corporate ownership pressures. When physicians are acquired by hospital systems or venture capital firms, clinical autonomy often diminishes. “They ain’t gonna let you do that,” Fred said, referring to the practice of prioritizing patient health over admissions and procedures.
The result is a primary care desert at precisely the moment primary care is most needed. Fred’s point was unambiguous: if you want to improve population health, you need more primary care access. You need more physicians oriented toward prevention, continuity, and the whole patient.
And ‘the system’ as currently designed actively discourages that.
==##==
** AI Use & Editorial Standards Disclosure. In producing this content, the authors employ AI language tools in a defined supporting role: (1) Research aggregation: surfacing relevant source material and authoritative references across peer-reviewed, institutional, the arts and journalistic databases; (2) Structural organization: proposing content architecture and draft sequencing; (3) Draft suggestion: generating candidate language for author review. The authors retain sole editorial responsibility for all published content. Every citation is independently confirmed as accurate and accessible prior to publication. No headlines, pull quotes, or factual claims are published without author verification. AI-generated language is treated as raw material then recast entirely in the authors’ established voices and subject-matter expertise before any content reaches publication. This workflow reflects the authors’ commitment to the standard that AI serve, not replace the author.
Healthcare leadership is rarely bold and too often ‘MIA’ when it comes the hard (risky) work of transforming our dysfunctional by design healthcare delivery and financing model about to implode on itself.
They’re generally risk averse and lazy bunch, preferring the hedge of ‘me too’ (what are my colleagues implementing?) strategies vs. the vision (and risk) of innovation’s upside potential when it comes to the transformational imperative to enable the triple aim (better care, superior outcomes at a lower per capita spend).
I’ve been in the ‘innovation space’ since the 80s in Southern California teaching doctors and hospital executives on the potential upside of managed care particularly as the model morphed away from closed loop systems (staff and group models) into a better fit with mainstream medicine, i.e, the IPA (Independent Practice Association).
Back in the day, HMOs were relegated to these limited and closed networks that primarily attracted 2nd and 3rd tier docs, often FMGs (foreign trained medical graduates) and the cohort within medicine that preferred the security of a salary at a staff or group model HMO vs. the entrepreneurial impulse to build a practice.
Amid current efforts to destroy vs. improve the ACA (Affordable Care Act) by defunding premium subsidies, here’s what we refuse to face, or that nobody wants to say out loud from the podium on social media, at networking parties or Congressional hearings:
With the advent of Maxicare’s ‘Window Project’ the penetration of mainstream medicine went full throttle to integrate HMOs into the growing pool of employer sponsored group health benefit plans, often side by side with ‘vote with your feet’ PPOs’. While also giving birth to the MSO (Management Services Organization) industry that provided essential infrastructure to assume and thrive under coordinated capitated payment terms.
The Lie We Keep Telling Ourselves
‘Medicare Advantage’ (MA) is NOT Medicare!
Let me translate: UnitedHealth coded harder, faster, and more aggressively than anyone else and got paid billions more because of it.
It’s not just a semantic quibble, nor splitting hairs per se. And it’s sure as hell not the technicality the MA lobby wants you to think it is.
Medicare Advantage is a term-limited contract with a private operator (MA plan) under Part C where CMS (the Centers for Medicare and Medicaid Services) ‘assigns’ the per member per year (PMPY) funds to the operator to administer Medicare-covered benefits under a capitation system. These terms and associated benefits are for one year. The operator can exit or change the contract terms, networks, formularies, utilization controls, and cost-sharing every single year. That’s not Medicare. That’s a commercial product wearing Medicare’s name tag.
As of January 12, 2026, the United States Senate just shoved that uncomfortable truth back into the national spotlight with a 105-page evisceration of UnitedHealth Group’s Medicare Advantage playbook.
Grassley Drops the Hammer: UnitedHealth and the Industrialization of ‘Diagnosis Capture’
Senator Chuck Grassley (R-Iowa), Chair of the Senate Judiciary Committee, released a majority staff report today that reads less like oversight and more like a forensic audit of a company that turned Medicare Advantage risk adjustment into its own profit-generating machine.
The thesis? UnitedHealth Group, the $400+ billion healthcare ‘too big to sail’ colossus that owns UnitedHealthcare, Optum, and effectively controls 10 million+ MA lives, has weaponized “diagnosis capture” including severity of illness/intensity of service upcoding at industrial scale.
In-home health risk assessments (HRAs) conducted by nurse practitioners whose job it is to find billable diagnoses
Secondary chart reviews by professional coders hunting for missed revenue opportunities
Pay-for-coding incentives to external clinicians – literally paying doctors to document more
Vertically integrated providers whose EHR workflows can be shaped by the parent company
AI-powered analytics identifying diagnosis opportunities where clinical thresholds are “squishy” (their word, not mine)
This isn’t a one-off compliance issue. This is the systemic architecture of a ‘healthcare borg’ that assimilates all material innovations intent on the transforming our paradigm from a fee-for-services, ‘do more to earn more’ model to one focused on the right patient, right care, right setting and time alchemy of a medical necessity driven model.
Grassley’s staff reviewed 50,000 pages of UnitedHealth documents including training materials, internal policies, software tools, audit protocols, etc., and concluded that UnitedHealth “turned risk adjustment into a major profit-centered strategy, which was not the original intent of the program.”
Industry publication Healthcare Dive reports that UnitedHealth “strategically captured a higher number of diagnoses and diagnosis codes than any other MA insurers – also resulting in higher CMS reimbursement than any of its peers.”
Now, UnitedHealth disputes the framing. They say their programs comply with CMS requirements and audits. Fine. But here’s the policy question that transcends any single actor:
Can a public program remain financially and clinically coherent when private plans are paid based on diagnoses, they are financially motivated to find?
OIG Already Told Us This – With Receipts!
If you want to know whether “diagnosis capture” is real, don’t read corporate press releases. Read watchdogs, including ACO Watch.
In October 2024, the HHS Office of Inspector General reported that diagnoses submitted only on HRAs and HRA-linked chart reviews, with no other service records tied to those diagnoses, drove an estimated $7.5 billion in MA risk-adjusted payments for 2023.
Read that again: Diagnoses that didn’t show up anywhere else in the encounter data still drove billions in payments.
STAT News’ coverage noted that UnitedHealth alone accounted for $3.7 billion of that $7.5 billion, almost half the total.
OIG’s point wasn’t “HRAs are always bad.” It was more damning: HRAs are vulnerable to misuse because they’re frequently administered by plans or vendors rather than a patient’s own treating clinicians.
The lack of any other follow-up visits, procedures, tests, or supplies for 1.7 million MA enrollees raises concerns that either:
The diagnoses are inaccurate (and thus the payments are improper), or
Enrollees didn’t receive needed care for serious conditions
Either way, taxpayers once again are the ‘bag holders’ for corporate greed..
MedPAC has been ringing the same alarm bells for years: MA risk scores remain higher than they would have been in traditional Medicare even after statutory adjustments, and coding intensity varies wildly across plans.
GAO documented years ago that coding differences can inflate risk scores and drive excess payments beyond what CMS adjustments have historically offset.
So, when a Senate report alleges a major payer optimized that vulnerability with uncommon scale and sophistication, it lands on pre-softened ground.
The Nursing Home Story: When Capitation Conflicts with Clinical Judgment
While Grassley’s report focuses on payment coding mechanics, there’s a second Senate track that’s even darker.
Senate Finance Committee leaders Ron Wyden (D-Ore.) and Elizabeth Warren (D-Mass.) have been investigating allegations related to UHG/Optum programs in nursing homes, specifically whether incentive structures designed to reduce hospital transfers create dangerous conflicts of interest.
A January 8, 2026 follow-up letter presses UHG for documents and details, citing heightened concerns and reported adverse outcomes, including at least three nursing home residents who allegedly died after being denied hospital transfers.
STAT reports that The Guardian’s December 2025 investigation spotlighted allegations that UnitedHealth’s cost-reduction programs may have resulted in deaths.
If the coding story is about who gets paid and why, the nursing home story is about something even more visceral:
What happens when the entity holding the capitation also influences whether a frail elder gets transferred to the hospital?
In managed care, “reducing unnecessary hospitalizations” can be good medicine. It can also be cost containment dressed up as care transformation. The line isn’t always bright which is exactly why Senate oversight matters here.
The Brand Problem: Stop Calling It “Medicare”
Now let’s talk about the part nobody wants to say out loud because it sounds too obvious:
If MA were truly “Medicare,” it wouldn’t need to borrow Medicare’s name to sell itself.
Yet the market reality remains: Consumers experience a daily blur of ads that imply they are “upgrading Medicare” rather than switching into a private plan with rules, restrictions, and networks.
So, here’s my position, plainly:
· MA is a private contract (Part C), not the Medicare program (Parts A & B under statute).
· Advertising should never use “Medicare” as a branding shortcut that obscures the private nature of the coverage.
· At minimum, any marketing that uses “Medicare” prominently should be required to state prominently, that it is a non-government plan option and not the Medicare program itself.
This is not anti-choice. It’s pro-informed consent.
The Selection Problem: Cherry-Picking Without the Cherry-Picking
MA plans are required to accept all applicants in their service area during appropriate enrollment periods, but “selection” doesn’t only happen through formal denial.
KFF’s analysis notes that people who enroll in MA spent $1,253 less per year in traditional Medicare before they switched, even after risk adjustment. That’s not MA making them healthier. That’s MA attracting healthier people. Let that sink in!
Research published in Health Affairs found that favorable selection into MA led to an average of $9.3 billion per year inoverpayments between 2017 and 2020.
KFF has also documented that people who disenroll from MA tend to have higher spending than similar beneficiaries who remain in traditional Medicare, consistent with risk dynamics and churn that can disadvantage higher-need individuals.
The Urban Institute’s comprehensive review concludes: “consistent and convincing evidence shows that favorable selection, after accounting for risk adjustment, is a key contributor to MA overpayment.“
When you combine favorable selection with coding intensity, you get a plausible recipe for a program that looks efficient while shifting financial pressure back onto the statutory Medicare program and taxpayers.
The Counterargument: MA Delivers ‘Value’ – Sometimes Real, Sometimes Theater
If we’re going to be credible, we must acknowledge what MA does offer:
An out-of-pocket maximum for Part A/B services (traditional Medicare does not have one unless paired with Medigap or other supplemental coverage)
Supplemental benefits (dental/vision/hearing and more) that many beneficiaries want and use
In many markets, lower premiumsand“bundle convenience,” including formulary (PBM) driven integration of Part D (the prescription drug plan)
Industry advocates also argue that some widely cited “overpayment” estimates are inflated by methodology and ignore program differences (like supplemental benefits and OOP – out of pocket- limits).
That’s the debate. But here’s the pivot:
Even if MA can deliver consumer value, it does not follow that “coding games” and “misleading branding” are acceptable collateral damage.
We can preserve consumer-facing benefits AND reform the incentives that distort coding, care, and communication.
What Reform Could Look Like (Without Blowing Up Choice)
Here’s a practical reform stack—built from watchdog findings and policy logic, not ideology:
1. Stop Paying for “HRA-Only” Diagnoses Without Corroboration
OIG’s findings make this the low-hanging fruit: If a diagnosis exists only in a plan-driven assessment and never appears in follow-up care or encounter records, it should not drive payment without additional evidence.
2. Strengthen RADV and Data Validation with Real Consequences
The MA payment engine runs on diagnosis data. Audits have to be scalable, timely, and consequential, or they become theater.
3. Align Risk Adjustment with Clinical Action, Not Just Documentation
If diagnosis capture is “real,” it should show up as care plans, monitoring, meds, referrals, or resource use. If it doesn’t, why is Medicare paying as if it does?
4. Truth-in-Advertising: Stop Calling MA “Medicare”
Make the distinction unavoidable in marketing:
“a Private plan option“
“Not the Medicare program”
“Plan networks and prior authorization may apply”
Plain-English trade-offs
5. Rebalance Incentives So Plans Win by Keeping People Well, Not by Finding Codes
Risk adjustment is necessary, but it shouldn’t be a profit center.
Bottom Line: The Medicare Brand Must Mean Something
The Senate’s scrutiny of UnitedHealthcare, paired with watchdog evidence on coding intensity, should be a wake-up call for policymakers, providers, and patients.
This is not a niche compliance squabble. It’s a structural integrity issue for a massive public-private hybrid that now covers tens of millions of older adults, including this author.
If you want to keep Medicare sustainable, you need two kinds of honesty:
Payment honesty (diagnoses should reflect reality and care), and
Marketing honesty (Medicare Advantage is not Medicare)
Because when a private contract markets itself as a public promise, and when diagnosis codes become a revenue stream, we don’t just risk overpayment.
We risk public trust.
And once that’s gone, good luck sailing anything – Medicare included.
==##==
** AI provided an assist via background research, organization and validation of claims as supported or challenged by authoritative 3rd parties, ie, academia, government, NGO or industry sponsored case studies.
Quick FAQ
Is Medicare Advantage the same as Medicare? No. Medicare Advantage (Part C) is offered by private insurers under contract with CMS; Original Medicare is the federal program (Parts A & B).
Why is MA under Senate scrutiny? Senate investigators are examining whether some MA practices—such as aggressive diagnosis capture for risk adjustment—may inflate payments, and whether certain care models create problematic incentives (e.g., nursing home hospital transfer decisions).
What is “risk adjustment” in MA? CMS pays plans more for members coded as sicker (higher risk scores) to discourage avoiding high-need patients—yet it creates incentives to maximize diagnoses.
Do MA plans have benefits Original Medicare doesn’t? Often yes—out-of-pocket limits for Part A/B services and supplemental benefits like dental/vision/hearing are common.
Gregg Masters, MPH, is a health policy analyst, public health and patient safety advocate and founder of ACOWatch.me. Follow him on social media @GreggMastersMPH or visit www.EndNMP.org or 2healthguru.wordpress.com for more analysis.
The news is monumental for the cannabis space and public health writ large. Here’s what actually happened today (Dec 18, 2025) and what the Trump cannabis Executive Order (EO) actually does – plus the 280E implications and the road ahead.
An interesting ‘sidebar‘ came via CMS Administrator Oz who indicated beginning Q2 2026 (April), CBD will be available for ‘free’ via physician order from ACOs, noting as well Medicare Advantage plans are ‘evaluating’ whether to include CBD in their supplemental benefits offerings to seniors as well.
We do live in interesting times!
Considering the relative underreporting of this signature event in the cannabis space, I’ve compiled a news summary and ‘explainer’ for your consideration with an AI assist in research and claim validation.
The news in plain English
President Trump signed an EO titled “Increasing Medical Marijuana and Cannabidiol Research” directing the Attorney General to complete the already-started federal rulemaking to move marijuana from Schedule I → Schedule III “in the most expeditious manner” (while staying within the Controlled Substances Act process). Source:The Washington Post+3The White House+3The White House+3
This is significant because it’s a White House-level push to break a procedural logjam: the Schedule III proposal has been pending since DOJ’s 2024 proposed rule and was sitting in the administrative hearing phase that got postponed. Source:Federal Register+2DEA+2
Directs the Attorney General to “take all necessary steps” to complete the Schedule III rescheduling rulemakingas fast as possible, consistent with 21 U.S.C. § 811 (the CSA scheduling process).
Directs White House legislative staff to work with Congress on updating the statutory definition around hemp-derived cannabinoid products (esp. “full-spectrum CBD”) and building a regulatory framework (e.g., THC-per-serving concepts).
Directs HHS/FDA/CMS/NIH to develop research methods/models using real-world evidence to improve evidence and standards of care around medical marijuana/CBD.
Includes standard language that it doesn’t create enforceable rights and must be implemented consistent with law/appropriations.
Important nuance: The EO is best read as an acceleration directive, not a magic wand that unilaterally “changes the schedule tomorrow.” The CSA still routes the change through the administrative rulemaking record. Source:The White House+2Federal Register+2
Does this eliminate 280E – and who benefits?
What 280E actually says
IRC § 280E disallows deductions/credits for businesses “trafficking in controlled substances”, “within the meaning of schedule I and II” of the CSA. This otherwise normal deduction of routine operating expenses has put cannabis dispensary operators (multi and single state) as a distinct competitive disadvantage. Source: Legal Information Institute
The key implication
So, if marijuana is finalized as Schedule III, 280E no longer applies to marijuana trafficking (because 280E is keyed to Schedule I or II, not III). Source: Legal Information Institute
Medical only, or recreational too?
Not medical-only. If marijuana is Schedule III federally, the 280E relief would generally benefit state-legal operators regardless of “medical vs adult-use” label, because 280E’s trigger is the schedule, not whether a state calls a sale medical or recreational. Source: Legal Information Institute
But: rescheduling does not federally legalize adult-use commerce; it just removes this specific tax penalty once the rule is final/effective. Source: The Washington Post+1
Timing: when would 280E relief actually start?
Not on EO day. It starts only after a final rule is issued and becomes effective (typically after Federal Register publication with an effective date). Until then, operators are still under the current Schedule I framework for federal tax purposes.
Why the EO matters (even though it’s “only” rescheduling)
If Schedule III is finalized, the high-impact wins are:
280E relief → ordinary business deductions return (rent, payroll, marketing, etc.), which can materially change cash flow and valuation math for operators. Source:Legal Information Institute+1
Research friction decreases vs Schedule I, potentially expanding clinical research and product development pathways. Source: The White House+1
It’s a federal acknowledgement of medical use, aligning more with current state realities—without ending federal control. Source: The White House+1
What it does not do
Even with Schedule III (and certainly with just the EO):
No federal legalization of recreational cannabis.
No interstate commerce greenlight for state markets.
No automatic SAFE/SAFER banking fix (banks still weigh federal illegality/risk; legislation is the clean solution).
No de-scheduling (removal from the CSA schedules entirely).
No broad criminal justice reform baked in (Editor’s note: some say the absence of AG Bondi at signing ceremony is a curious absence?).
(Those limits are why some coverage frames this as big-but-not-the-finish-line.) Source: AP News+1
What’s next (near-term roadmap)
DEA/DOJ completes the administrative process: resolving the stalled posture and moving to a final agency action. The rule has been pending since DOJ’s May 2024 proposed rule, and the hearing phase was postponed. Source: Federal Register+2DEA+2
Final rule published (Federal Register) + effective date.
Litigation risk / judicial review: major federal changes like this often draw court challenges, which can affect timing and certainty.
Parallel track: Congress (banking, taxation, states’ framework, descheduling bills) if political will exists.
Road to full de-scheduling (the real “endgame”)
De-scheduling generally requires Congressional action (amending the CSA) or a far more sweeping administrative move than the current Schedule III track – and it also runs into broader regulatory architecture questions (FDA framework, commerce, taxation, public safety, treaties). Practically, most paths to true normalization run through Congress.
Bottom-line?
The December 18, 2025 signing ceremony delivered a headline that – depending on where you sit – reads like long-overdue common sense, political triangulation, or a regulatory Rorschach test: President Donald J. Trump signed an executive order titled “Increasing Medical Marijuana and Cannabidiol Research.”Source:The White House
Here’s the crucial nuance right up front: the Executive Order (EO) does not itself reschedule marijuana. Under federal law, rescheduling happens through a formal rulemaking process anchored in the Controlled Substances Act (CSA) – not by presidential decree. What the EO does is direct the Attorney General to “take all necessary steps” to complete the ongoing rulemaking to move marijuana from Schedule I to Schedule III “in the most expeditious manner in accordance with Federal law,” explicitly referencing 21 U.S.C. § 811.Source:The White House+1
If you’re running a state-legal cannabis business – or tracking one from the investor side – the part that lands like a thunderclap is the tax angle:Schedule III would typically remove cannabis from the scope of IRS Code Section 280E, the federal provision that disallows ordinary business deductions for “trafficking” in Schedule I or II controlled substances. Source:Legal Information Institute+1
Let’s unpack what’s actually in the EO, why it matters, what it likely means for 280E (medical and adult-use), and what “next” looks like on the road to full de-scheduling.
What the Executive Order actually says (and does)
The EO frames federal cannabis policy as lagging behind widespread medical use and clinical reality—particularly around chronic pain, seniors, and veterans. It argues that Schedule I status has “impeded research” and left patients and clinicians without adequate guidance. Source:The White House
The operational heart of the order is Section 2, which sets out three main directives:
Expedite Schedule III rescheduling (Attorney General). The EO instructs the Attorney General to move the rescheduling rulemaking forward “in the most expeditious manner” under the CSA, citing 21 U.S.C. § 811 – the statute that governs adding, removing, or transferring substances between schedules through rulemaking and hearings. Source: The White House+1
Push a legislative/regulatory pathway for hemp-derived cannabinoids and full-spectrum CBD (White House Deputy Chief of Staff + Congress). The EO calls for working with Congress to update the statutory definition and establish a regulatory framework, including THC-per-serving limits and ratio considerations. Source: The White House+1
Accelerate research methods and “real-world evidence” (HHS, FDA, CMS, NIH). It directs federal health agencies to develop research methods—explicitly including real-world evidence—to inform standards of care and improve lawful access to hemp-derived cannabinoid products. Source: The White House+1
The EO also explicitly references the existing federal rescheduling process already in motion: DOJ issued a proposed rule in May 2024; the proposal drew nearly 43,000 public comments; and it is “awaiting an administrative law hearing.” Source: The White House+1
That matters because it signals the administration isn’t “starting a new process.” It’s trying to finish an already-started one – faster.
The rescheduling process is rulemaking on the record – no shortcuts
Under the CSA, the Attorney General (delegated to DEA) can transfer a drug between schedules via rulemaking, and the process includes notice, comment, and an opportunity for a hearing. Source: U.S. Code+1
The DOJ/DEA proposed rule published in May 2024 is the backbone: it proposes moving marijuana from Schedule I to Schedule III, relying on HHS’s medical/scientific assessment (which the proposal describes as deserving significant deference). Source: Federal Register+1
Also important: the proposed rule is unusually candid about what rescheduling does not do.
It does not federally legalize marijuana.
Criminal prohibitions under the CSA still apply.
Products containing “marijuana” under the CSA remain subject to the Federal Food, Drug, and Cosmetic Act (FDCA), including FDA approval requirements for lawful interstate commerce absent an IND framework. Source: Federal Register
So: Schedule III is a big change – but it’s not “legalization,” and it’s not “de-scheduling.”
The 280E question: medical only, or does adult-use benefit too?
You asked the question that matters to operators’ cash flow:
Does this eliminate 280E for medical dispensaries only, or do recreational dispensaries benefit too?
If marijuana is finalized into Schedule III, the benefit is not limited to “medical-only” dispensaries. The reason is simple: 280E is keyed to Schedule I and II substances – not to whether a state labels cannabis “medical” vs “adult-use.” Source: Legal Information Institute+1
The statutory text of 26 U.S.C. § 280E denies deductions/credits for a trade or business that traffics in controlled substances “within the meaning of schedule I and II” that are prohibited by federal law or the law of the state in which the business operates. Source:Legal Information Institute
That means:
Schedule I/II status is the trigger.
If marijuana moves to Schedule III, it is no longer a Schedule I/II substance.
Therefore, 280E generally should no longer apply to businesses “trafficking” in marijuana—even though marijuana would still be federally controlled and the CSA would still criminalize unauthorized distribution. (280E doesn’t care about “illegality” in the abstract; it cares about illegality involving Schedule I/II.) Source:Legal Information Institute+1
The Congressional Research Service (CRS) describes 280E as denying deductions and credits for trafficking in Schedule I/II substances and explains why it has applied to state-legal marijuana businesses while marijuana remains Schedule I. Source:Congress.gov
Bottom line:Both medical and adult-use cannabis operators would generally benefit from the end of 280E disallowance once – and only once – marijuana is officially moved out of Schedule I/II. (I’m emphasizing “once” because the EO alone does not change the tax treatment today.) Source:The White House+1
Still true even after Schedule III: cannabis businesses would still face complex federal-state contradictions (and likely continued banking and interstate-commerce constraints), but the tax math changes materially when ordinary and necessary business expenses become deductible again. The Federal Register notice itself flags that 280E is a major economic consideration in the rule’s impact analysis. Source: Federal Register
Quick note (not tax advice): even under 280E, businesses have typically been able to reduce gross receipts by cost of goods sold (COGS) – the real pain is losing ordinary deductions (rent, payroll, marketing, admin, security, etc.). That’s why Schedule III is viewed as an immediate profitability lever.
Why this EO is significant (even though it doesn’t “legalize”)
1) It tightens the federal narrative around “medical use” and “research”
The EO is explicitly framed around medical marijuana and CBD research, and it leans into the health system’s reality: chronic pain is widespread (CDC reports 24.3% of U.S. adults had chronic pain in 2023). Source: CDC
That framing matters because re-scheduling requires findings about medical use and abuse potential under the CSA’s criteria. Source:U.S. Code+1
2) It puts “real-world evidence” on the table
Traditional cannabis research has been constrained for decades by Schedule I barriers and supply bottlenecks. The EO’s push toward real-world evidence isn’t just a research preference—it’s an implicit acknowledgment that millions of Americans are already using these products, and clinicians need better data to counsel patients.
The National Academies’ landmark 2017 report found substantial evidence supporting cannabinoids’ effectiveness for chronic pain in adults, while also documenting risks and research gaps. Source:National Academies+1
3) It spotlights CBD product integrity and safet
CBD is widely used, but product labeling accuracy and contamination remain uneven across an under-regulated marketplace. Peer-reviewed analyses have found widespread mislabeling in commercially available CBD products. Source:PMC+1
The EO’s CBD provisions—especially talk of THC-per-serving limits and a clearer regulatory framework—signal a federal attempt to reduce harm from today’s “Wild West” consumer cannabinoid market. Source:The White House+1
4) It is (also) an economic policy move – via 280E
Let’s be honest: the fastest, most measurable impact of Schedule III isn’t a new randomized trial. It’s a cleaner P&L.
News coverage today highlights that rescheduling could deliver meaningful tax relief by ending 280E’s punitive treatment for cannabis businesses. Source:AP News
What happens next: the near-term roadmap
Here’s the “what’s next” sequence in plain English:
Administrative law hearing + record building The EO itself says the proposed rule is awaiting an administrative law hearing. Source:The White House+1
DEA decision + final rule After the hearing process and review of the administrative record, DEA can publish a final rule (or withdraw/modify the proposal). The Federal Register proposal underscores that rescheduling must happen through formal rulemaking on the record. Source:Federal Register
Effective date + downstream compliance If finalized, marijuana would become Schedule III under federal schedules. At that point, the 280E issue changes in a very practical way. Source:Legal Information Institute+1
Legal challenges are likely Given the stakes and polarization, expect litigation – either challenging the procedure, the scientific basis, or treaty compliance logic. The proposed rule itself spends notable space discussing how Schedule III could be made consistent with U.S. international treaty obligations through additional controls. Source:Federal Register
And after Schedule III: the longer road to “full de-scheduling”
If Schedule III is the on-ramp, de-scheduling is the freeway interchange that still requires legislative engineering.
De-scheduling can happen in two broad ways:
Path A: Administrative (harder)
In theory, DEA could initiate a rulemaking to remove marijuana from control. In practice, de-scheduling raises deeper questions – especially around international treaty obligations and how the U.S. would structure controls absent CSA scheduling. The DOJ proposal already signals treaty constraints are non-trivial even for Schedule III. Source:Federal Register
Path B: Congressional (more direct, still politically difficult)
Congress can amend the CSA, create a federal regulatory framework for cannabis, address interstate commerce, taxation, public health guardrails, advertising, product standards, and banking. In other words: Congress can do what patchwork state markets can’t create coherence.
Even if you’re “team de-schedule,” Schedule III may be the pragmatic bridge: it normalizes medical research pathways and reduces the tax distortion that has functionally subsidized the illicit market by kneecapping compliant operators.
The public health lens (because this is ACOwatch)
As a public health guy, I can’t help noticing what this EO is – and isn’t.
It is not an endorsement of “everyone should use cannabis.” It’s an administrative acknowledgment that millions already do, many for pain and symptom management, and our federal research posture has been out of step with reality. Source:The White House+1
The evidence base is evolving and nuanced. For chronic pain, data suggest cannabinoids may provide small to modest improvements for some patients and some conditions, with meaningful variability and real adverse effect considerations. Source:BMJ Open+1
For ACOs and value-based care organizations, the more interesting question is less “culture war” and more:
Can better evidence, tighter product standards, and rational tax policy reduce harm, improve outcomes, and shrink the gap between what patients do and what clinicians can responsibly guide?
That’s the promise the EO gestures toward – if the bureaucracy follows through and if Congress eventually does its job.
Key takeaways for operators, investors, and clinicians
The EO is real and specific. It directs the AG to expedite Schedule III rulemaking and pushes federal agencies toward research and cannabinoid regulatory clarity. Source:The White House+1
It does not reschedule marijuana by itself. Rescheduling still requires DEA rulemaking, hearing processes, and final publication. U.S. Code+1
If Schedule III is finalized, 280E relief is not “medical-only.” 280E is tied to Schedule I/II, not to state program labels. Adult-use businesses would generally benefit too. Source:Legal Information Institute+1
Schedule III is not legalization. CSA prohibitions still apply; FDCA constraints still matter; and federal-state contradictions don’t vanish overnight. Source:Federal Register
De-scheduling is a bigger lift. Expect Schedule III (if finalized) to be a waypoint—not the destination.
**Disclosure and guardrails
This post is compiled by Gregg Anthony Masters, MPH, with an AI assist in policy research, analysis and public health commentary with authoritative third-party support for or challenges to unsubstantiated claims. It is not legal, tax, or investment advice. If you operate in the space, talk to counsel and a tax professional who lives and breathes cannabis compliance.
As producer or executive producer of six shows, both live and on demand, for Healthcare NOW Radio, including our most recent launch ‘Inside the Revival‘
we (the hosts and producers) were asked for our ‘Open Mic’ predictions for 2026 as follows:
What major event, transformation, or innovation in 2025 had a lasting impact on healthcare, whether positive or negative, and is likely to shape its future trajectory?
Pasted below is my one paragraph version, followed by a ‘long form‘:
The singular “impact event” of 2025 has been the politicization and destabilization of U.S. public health leadership at the very moment competence and continuity are most needed, against a backdrop of a structurally mispriced “sickcare” economy: in 2023 the U.S. spent about $4.9T on health care (≈ $14,570 per person; 17.6% of GDP) while federal public health spending fell sharply as pandemic-era funds expired (down 58.3% from $90.2B in 2022 to $37.6B in 2023), and CDC’s FY2025 budget request was $9.683B – a rounding error compared with the trillions spent treating disease after it matures. That underfunded prevention and surveillance backbone has now been hit by operational and governance shocks: USAID was dismantled following the 2025 foreign-aid review (with courts finding DOGE-linked actions likely unlawful), impairing a core global health delivery and surveillance apparatus whose disruption is associated with catastrophic projected mortality (including Lancet-linked estimates warning of >14 million additional deaths by 2030 under severe cut scenarios – think the ‘BBB’ Medicaid and Medicare cuts and ACA premium credit defunding), while immunization governance was destabilized when HHS removed all 17 ACIP members on June 9, 2025 – an action with real-world implications because ACIP recommendations are tightly linked to vaccine coverage and access across payers. Bottom line: the nation’s public health infrastructure = already treated as a political punching bag and fiscal afterthought relative to the acute care “non-system”- is perilously compromised and may take a generation to rebuild; for the full long-form, sourced analysis and timeline, see my post on ACOwatch.com. – Gregg Anthony Masters, MPH, Managing Director, Health Innovation Media
Long Form
The singular “impact event” of 2025 has been the politicization of U.S. public health leadership at precisely the moment when competence and continuity matter most – because public health is not a branding exercise; it is operational infrastructure.
Start with the structural imbalance. In 2023, the U.S. spent $4.9 trillion on health care- about $14,570 per person – and health spending consumed 17.6% of GDP.
That is the financial footprint of an acute, downstream “sick-care” model. Meanwhile, federal public health spending fell sharply as COVID-era funds expired dropping 58.3% from $90.2B (2022) to $37.6B (2023).
Even the CDC’s FY2025 budget request was $9.683B – a ’rounding error’relative to the trillions spent treating late-stage disease.
Against that backdrop, public health has been dealt a potentially lethal blow – not only through chronic underinvestment, but through destabilizing governance and dismantling core capabilities.
First: USAID
On January 20, 2025, the White House issued Executive Order 14169, initiating a foreign aid review and pause. In the wake of that process, USAID was dismantled, according to the Congressional Research Service’s overview of the 2025 restructuring.
Separately, a federal judge ruled that DOGE’s reckless dismantling of USAID likely violated the Constitution and blocked further cuts.
Whatever one’s politics, this is not “efficiency” – it is the impairment of a core global health delivery and surveillance apparatus, executed at speed by clueless DOGE actors with limited operational insight into what USAID does, how programs are implemented, and how health security risk is managed.
The downstream human cost is not hypothetical – in my book it’s borderline criminal. A Lancet-reported analysis warned that severe USAID funding cuts could contribute to more than 14 million additional deaths globally by 2030, including millions of children under five.
When you break global disease surveillance, reporting control practices (HIV, TB, malaria, maternal-child health, outbreak readiness), you don’t just harm “over there.” You increase the odds of delayed detection, disrupted containment, and cross-border spread – problems that always return. Think the iconic Fram oil filter commercial: where a mechanic holds up a new oil filter opining ‘you can pay me now (preventively) or pay me later‘ (in the shop).
Second: immunization governance and trust
On June 9, 2025, HHS announced it removed all 17 sitting members of ACIP. CDC later stated the 17 were replaced with eight new, shall we say more aligned with the Secretary of Health and Human Services anti-vax ideology, members.
This matters because ACIP is not symbolic: ACIP recommendations are tightly linked to vaccine access and coverage. Federal law generally requires most private plans to cover ACIP-recommended adult immunizations without cost-sharing, and KFF documents how ACIP recommendations function as a key trigger for coverage requirements.
Destabilizing that system invites confusion, coverage churn, and reduced uptake – fuel for outbreaks in an era when vaccination rates and trust are already strained. As a lead monitoring and declaring outbreaks in K-12 school districts for San Diego County, the trust of the public was a key driver of both trust and in the efficacy of the pandemic response (both NPI, non-pharmaceutical interventions and mass immunization efforts).
Bottom line: the management of our aggregate public health infrastructure is perilously compromised by ‘leaders’ at HHS, CMS, CDC, FDA and NIH who value the ideology over science mantra of the ‘charlatan in chief” RFK. Jr. We have a nation that can mobilize trillions to treat disease after it ‘matures’, yet repeatedly treats prevention, surveillance, and preparedness as foolishly expendable line items – until the next emergency arrives.
The consequences of dismantling USAID capabilities and destabilizing evidence-based advisory systems will not be measured in headlines; they will be measured in avoidable morbidity and mortality, domestically and globally.
It will likely years – possibly a decade or more – to rebuild durable surveillance, preparedness capacity, and the credibility required for effective public communication for potentially “unpopular” but necessary interventions.
Some of you may have heard about the whining by UnitedHealthcare’s leadership on a recent earnings call which included the required ‘management’s discussion or operating results and market conditions’ analysis. A BIG WHAAAA!
Overfunded since inception and having perfected the art of ‘upcoding‘ (i.e,, severity of illness and intensity of medically necessary services) Medicare Advantage (MA) operators with often market-specific and generous redistribution of the Center for Medicare and Medicaid Services (CMS) funds thus enabling Zero premium plans with expanded benefits, I’m totally fed up with the relentless ‘ad copy’ of my current health plan (KP San Diego) where I’ve been a loyal member and advocate of their ‘best in class’ IDN status and outcomes performance. They are NOT, and my journey into ‘e-patient‘ hood affords me this opportunity to opine in public.
So, here’s the first installment:
Prompt
I am 72-year-old man in good health. Open enrollment for Medicare ends tomorrow (12/7/2023). I need to make a decision whether to dis-enroll from a Medicare advantage program and return to statutory Medicare, not a term based, private contract with a Medicare advantage operator. I was recently diagnosed with prostate cancer with a Gleason score of 7 (3+4) and am in active monitoring & surveillance (including periodic PSA, mpMRI & targeted biopsies) and am not under treatment, yet. What are the pro’s and con’s of staying with my current health plan (Kaiser Permanente, San Diego) vs. opting for Medicare plus a supplement? What are my best choices? Do you need additional context or prompting? Do you understand?
ChatGPT
I understand your situation and the importance of making an informed decision about your Medicare options, especially in light of your recent prostate cancer diagnosis. Here’s a general overview of the pros and cons of Medicare Advantage plans versus Original Medicare with a Supplement (Medigap) plan, particularly in the context of your condition and current health plan with Kaiser Permanente in San Diego.
Medicare Advantage (like Kaiser Permanente):
Pros:
All-in-One Plan: Medicare Advantage plans often include Part D (prescription drug coverage) and may offer additional benefits like dental, vision, and wellness programs not covered by Original Medicare.
Cost-Capping: These plans usually have an out-of-pocket maximum, which can help manage costs.
Provider Networks: Plans like Kaiser Permanente often have a network of doctors and facilities, ensuring coordinated care and sometimes easier appointment scheduling.
Cons:
Limited Provider Networks: You may be restricted to doctors and facilities within the Kaiser network, limiting your choices for specialists, especially if you need specialized cancer treatment.
Referrals Required: Some plans require referrals for specialist visits, which might delay access to care.
Plan Restrictions: Some treatments or medications might not be covered, or may require prior authorization.
Original Medicare with a Supplement Plan:
Pros:
Wider Network: You have the flexibility to see any doctor or specialist that accepts Medicare, which can be beneficial for specialized cancer care.
No Referrals: Generally, no referrals are needed to see specialists.
Predictable Costs: Supplemental (Medigap) plans can help cover Medicare Part A and B deductibles, co-insurance, and other out-of-pocket costs, making expenses more predictable.
Cons:
Additional Premiums: You’ll likely pay a premium for both Medicare Part B and the Medigap policy.
Separate Drug Plan: You’ll need to enroll in a separate Medicare Part D plan for prescription drugs.
Potential Gaps: Some Medigap plans don’t cover extras like dental, vision, or wellness programs.
Considering Prostate Cancer Treatment:
Access to Specialists: With Original Medicare and a Supplement, you might have more flexibility in choosing specialists for your prostate cancer treatment.
Coverage for Treatments: Check the specific coverage details for cancer treatments under both options to understand potential costs and restrictions.
Making Your Decision:
Compare Costs: Consider premiums, deductibles, co-pays, and out-of-pocket maximums.
Evaluate Provider Network: Ensure your preferred doctors and hospitals are covered and consider the ease of access to specialists.
Review Drug Coverage: If you’re on medications, check how they’re covered under each option.
Consider Future Health Needs: Think about potential changes in your health and how each plan would accommodate those needs.
Given your specific health situation, it’s crucial to consider how each option would cover your ongoing monitoring and any potential future treatments for prostate cancer. Additionally, it might be beneficial to consult with a healthcare advisor or a Medicare specialist who can provide more personalized advice based on your health status and needs.
Please remember that this is a general overview and not personalized medical or insurance advice. It’s important to review the specific details of your current plan and compare them with the benefits offered under Original Medicare plus a supplement.
You
continue. if i dis-enroll from current health plan and given the current prostate cancer diagnosis, will I qualify for a Medicare supplement via community rating? Or will I be medically underwritten and potentially denied coverage? And will the rate be adjusted to reflect pre-existing conditions? Do you understand or need further prompting?
ChatGPT
Yes, I understand your question regarding eligibility and rates for a Medicare Supplement (Medigap) plan after disenrolling from a Medicare Advantage plan, particularly in the context of your current prostate cancer diagnosis. Here are the key points to consider:
Medigap Eligibility and Underwriting:
Guaranteed Issue Rights: Normally, when you first enroll in Medicare Part B at age 65 or older, you have a 6-month Medigap open enrollment period where you can buy any Medigap policy sold in your state without medical underwriting. During this period, you cannot be denied coverage or charged more due to pre-existing conditions.
Switching from Medicare Advantage to Medigap: If you are in a Medicare Advantage Plan, you can switch to Original Medicare with a Medigap policy under certain conditions. These conditions generally include moving out of your plan’s service area or if the plan stops providing care in your area. However, these situations would grant you a Special Enrollment Period with guaranteed issue rights for a Medigap policy.
Medical Underwriting Outside of Protected Periods: If you’re switching from Medicare Advantage to Medigap outside of these specific periods, insurance companies may use medical underwriting. This means they could charge higher premiums based on your health status, or potentially deny coverage due to pre-existing conditions.
Community Rating in Some States: Some states, like New York and Massachusetts, use “community rating” for Medigap policies, where premiums are not based on age or health status. In these states, your prostate cancer diagnosis would not affect your premium rates.
California Rules: Since you are in San Diego, California’s rules for Medigap plans apply. California uses a “birthday rule,” allowing Medicare beneficiaries to switch to a Medigap policy with the same or lesser benefits during the 30 days following their birthday each year, without medical underwriting. However, this is only applicable if you already have a Medigap policy.
Considering Your Situation:
Current Health Status: Given your prostate cancer diagnosis, if you are outside of a guaranteed issue period or special enrollment period, there is a risk of higher rates or denial of coverage due to medical underwriting.
Advice: It’s highly recommended to consult with a Medicare specialist or insurance advisor who can provide detailed information based on your specific situation, including your current health status and the rules in your state.
Remember, these are general guidelines and may not cover every nuance of your situation. It’s important to get personalized advice before making a decision, especially given the complexities surrounding health conditions like cancer and their impact on insurance eligibility and rates.
You
continue: create a blog post titled: “Medicare Open Enrollment: To Dis-enroll or Not? Searching For Answers with an AI Assist”. Use the above query and explanation. Create in witty yet professional tone. Do you understand or need further prompting?
ChatGPT
Absolutely, I understand your request. Here’s a blog post based on our previous discussion:
Medicare Open Enrollment: To Dis-enroll or Not? Searching For Answers with an AI Assist
Welcome to the rollercoaster ride of Medicare open enrollment! It’s that time of the year when we, the silver-haired brigade, scratch our heads, pore over pamphlets that might as well be written in Klingon, and try to make sense of our health insurance options. Fear not, dear reader, for today we have a secret weapon in our arsenal – an AI assistant (that’s me, by the way)!
The Great Debate: Medicare Advantage vs. Original Medicare with a Supplement
Imagine you’re at a health insurance buffet. On one table, we have Medicare Advantage plans, like the one from Kaiser Permanente in sunny San Diego. It’s like a combo meal – a bit of everything in one package. On the other table, there’s Original Medicare with a side dish of Medigap (Supplement) plans. More à la carte, you pick and choose what suits your palate.
The Medicare Advantage Plate: A Mixed Bag
Pros:
Convenience: These plans roll your Medicare Parts A, B, and often D into one. It’s like getting a burger, fries, and a soda in one go.
Cost Caps: There’s a limit on out-of-pocket expenses. It’s like knowing you won’t spend more than $20 on your meal, no matter how many extra fries you grab.
Extra Goodies: They often throw in benefits like dental and vision – the cherry on top.
Cons:
The Network Maze: You might be restricted to their network of doctors. It’s like only being able to eat at restaurants in one neighborhood.
Referral Hoops: Need a specialist? Get ready to jump through some referral hoops.
Coverage Caveats: Some treatments or drugs might not be on the menu.
The Original Medicare with Supplement Platter: Customize Your Meal
Pros:
Freedom of Choice: See any doctor who accepts Medicare. It’s like having a pass to dine at any restaurant in the city.
No Referrals Needed: Straight to the specialist you go, no pit stops.
Predictable Costs: Supplement plans can cover those pesky out-of-pocket costs, making your expenses more like a fixed-price menu.
Cons:
Extra Bills: You’re paying for two plans – think of it as buying a main dish and a side separately.
Drug Plan Detour: You’ll need a separate plan for medications – yes, another dish to order.
Extras Not Included: Want dental or vision? That’s another order you’ll need to place.
The Plot Twist: A Prostate Cancer Diagnosis
Here’s where the plot thickens. With a recent prostate cancer diagnosis and a Gleason score of 7, the decision gets more nuanced. You want a plan that covers your needs, like a chef who can cater to your specific dietary requirements.
Dis-enrolling and Medigap: Navigating the Maze
If you’re thinking of waving goodbye to your Medicare Advantage plan and waltzing over to Original Medicare with a Medigap policy, hold your horses. There are things to consider:
Guaranteed Issue Rights: This is your golden ticket to get a Medigap plan without being penalized for health issues. But it’s time-sensitive.
Medical Underwriting: Miss the golden period, and insurers might look at your health as closely as a chef inspects produce. This could mean higher rates or a polite “no thank you” to offering you a plan.
California’s Birthday Rule: In the Golden State, you get a chance to switch Medigap plans around your birthday without medical underwriting. It’s like getting a free dessert on your special day – but only if you already have a Medigap plan.
The Verdict?
It boils down to personal preference, health needs, and a bit of timing. Think of it like choosing between a set menu and a build-your-own meal. Each has its perks and drawbacks.
So, dear readers, as you navigate these choppy waters of Medicare decisions, remember: it’s about finding the right fit for your health and lifestyle. And while I, your AI assistant, can provide a map, it’s always wise to consult a human expert – think of them as your personal health insurance sommelier.
Happy enrolling! May your health insurance choices be as satisfying as your favorite meal.
It’s been quite some time that I’ve updated this site though not for a lack of news. Yet some 434 posts later following the rollout of the Affordable Care Act, the signature, and against all odds accomplishment of then President Barack Obama, I thought I’d update both subscribers and followers of the blog including a number of generous guest contributors.
Since SARS-CoV-2 entered our collective consciousness in March 2020 as a global pandemic and has reconfigured any sense of ‘normal’ , like many of you, I have been reflecting on the nature and meaning of this uniquely challenging journey.
Today, I celebrate 71 years of existence on this ‘pale blue dot‘. Yet, it doesn’t feel like a celebratory moment. With seemingly everything upside down from ‘truthiness’ and ‘alternative facts’ driving wedges of relentless tribalism between people and moments that matter, I am revaluing where are how I spend my time.
As Nick van Terheyden MD aka ‘Dr Nick’ once offered:
Gregg you may want to try the 5/25 approach. Where you concentrate on the 5 of the twenty five priorities on your to-do list.
As a public health graduate from the UCLA School of Public Health in the 70s (post HMO Act) and following serial up and down c-suite cycles (peppered by severe bouts of clinical depression) leading health system participation in managed care spanning, community and tertiary hospitals in the ‘non-profit’ and‘proprietary’ sectors for nameplate health system parents and academic medical centers, I feel quite discouraged that the more things‘change’in healthcare delivery and finance, the more things remain the same. Or as otherwise put legacy momentum is likely to prevail as the status quo – or as our industry once characterized by Esther Dyson as a‘calcified hairball’ – is likely to resist or assimilate all meaningful innovation (think population health or value based care).
In anticipation of the enshrinement of accountable care organizations or ‘ACOs’ in healthcare innovation lexicon for the foreseeable future, in addition to ACOwatch.com, I acquired a range of digital assets to potentially develop, co-develop, lease or sell.
So years ago, when twitter burst into the landscape of an emerging digital health economy (circa 2008/09), sitting in a Health 2.0 annual gathering and listening to the presentations two ideas came to mind as cute twitter handles that might host and gain conversational traction in health policy circles and the soon to be emerging tweetchats.
twitter ‘jail’!
They included @HealthcareBorg (a somewhat witty ‘resistance is futile’ play on the then very popular Healthcare Blog, courtesy of Matt Holt, et al). The other session generated name ID was @ReplaceMyMD (inexplicably suspended by content managers at twitter – including @ACOwatch, @DocTweets, @HospitalTweets, @TweetHealth, @PreferredPharma, @ACOalliance, @CancerCenterTV, @JustOncology, @BioMarkersToday and many others) which I thought was more than cute given the bifurcation of consumer friendly (from a retail POV, ie, app savvy and tech enabled) tools likely to flood the market to enable the essential literacy to navigate a progressively complex health policy environment that assumed the consumer with high deductible health plans would be interested in ways to shelter their out-of-pocket (cost shifting) spending from increasing co-pays, co-insurance and deductibles unfortunately enshrined in the ACA as an offset to the total cost of the Act.
Available ACO Assets Include:
ACOalliance.com
ACOroundtable.com
ACOregistry.com
ACOcor.com (anyone remember PhyCor??)
AccountableCare.Center
ACOchat.org
AccountableCare.Solutions
So with perhaps with more than a tinge of ‘battle fatigue’and the increased participation of smart, motivated, and confident digital natives convinced value based healthcare is within sight, I am pivoting away from active work in this domain.
Instead I am concentrating on developing services for popupstudio.productions offering onsite ‘pop-up studios’to simultaneously livestream conference, exhibition, tradeshow or event specific ‘user group’ streams across most major social channels including: YouTube, FaceBook Live, LinkedIn or enterprise/organization website(s).
My 2nd pivot is to concentrate on both B2B and B2C educational messaging in the emerging medical cannabis marketplace and the closely aligned and re-invigorated research activity into the therapeutic benefits of psychedelics.
If you have an interest in working with any of the ACO themed domains above, please follow then ping @GreggMastersMPHvia DM on twitter.
Some eight plus years in, ACOs are still earning their ‘shared savings‘ industry ‘sea-legs’.
While they remain a central actor of transformation from volume to value birthed by the ACA for both the public (Medicare and Medicaid) and private (commercial health plans) sectors, the results are continuing to build.
The skeptics think they’re at best transitional vehicles toward more fully expressed and mature risk bearing entities with culture and risk infrastructure suitable to participate in an MA plan.
Below are are two recent articles that dive into the results:
CMS posted the dataset on September 14, 2020 for program year 2019 for both financial and quality performance:
CMS released financial and quality performance results for Performance Year (PY) 2019 and PY 2019A. PY 2019 includes the performance periods beginning January 1, 2019 and ending June 30, 2019 as well as the performance period beginning January 1, 2019 and ending December 31, 2019. PY 2019A refers to the performance period beginning July 1, 2019 and ending December 31, 2019.