by Gregg A. Masters, MPH
It may come to a surprise for some that ‘healthcare innovation‘ has been in play for quite some time albeit not fueled by a culture of hacking or disrupting legacy operations principally via technology. Unfortunately a veritable acronym soup of mostly failed initiatives under varying degrees of public, private partnership (PPP) collaborations have been largely unsuccessful albeit with momentary pauses to the growth rate of healthcare or its underlying medical care cost (MCC) inflation.
When I started in the space national healthcare spend represented 6% of GDP (today, last reported at 17.9%) and many of the same stakeholders were then complaining about its unsustainable trajectory, un-affordable health insurance premiums, wide variations in quality and the uneven access created by a confusing universe of often conflicting payor class (or ‘book of business’) driven reimbursement requirements.
Back then, we witnessed the launch of professional standards review organizations (PSROs) who’s mission was to develop what many referred to as ‘cookbook’ medicine guidelines for purposes of utilization review and medical necessity determinations that health maintenance organizations (HMOs), and to a lesser degree preferred provider organizations (PPOs), deployed via a range of products introduced as ‘managed healthcare’.
HMOs were seen as ‘closed loop‘ systems principally built upon ‘staff models’ where physicians were health plan employees (think Kaiser Permanente, though technically a ‘group’ vs. staff model), Cleveland Clinic, or Geisinger Health plan and thus had not penetrated either mainstream medicine nor commercial market customers (employers, coalitions, multiple employer trusts or purchasing cooperatives, etc.) that Aetna, Cigna, United and Blue plans designed, underwrote and marketed a range of self funded and fully insured insurance products. Both Medicare and Medicaid remained untapped ‘managed markets’ as well. Thus the lion’s share of both public and private markets were in traditional domain of unbridled fee-for-services medicine based on usual and customary pricing or payment schedules tied to conversion factors associated with resource based relative value units (RBRVU).
This began to change with the introduction of independent practice associations (IPA) supported by a competent management services organization (MSO) or physician practice management company (PPMC) providing back office support needed for private physicians in independent practices to contractually engage with health plans. This pivot began an era shifting risk from the health plan to the contracted provider network via a range of reimbursement models.
From modest withholds on negotiated fee-for-services schedules, to global or service tiered per diem’s, case rates or in the most aggressive arrangements an outright delegation of global (including hospital) or partial (professional services only) risk. The latter typically involved mature multi-specialty or primary care group practices with professional management, supporting culture and the associated infrastructure to bear the risk burden.
 The aggregate impact of the frenzy that followed by huge market share gains in the HMO space and a correspondingly similar growth in the PPO market was a medical trend reduction and at one point temporary negative decline in healthcare and medical cost inflation indices relative to GDP the late 80s to mid 90s.
The aggregate impact of the frenzy that followed by huge market share gains in the HMO space and a correspondingly similar growth in the PPO market was a medical trend reduction and at one point temporary negative decline in healthcare and medical cost inflation indices relative to GDP the late 80s to mid 90s.
Yet, the cultural flash point was perhaps best captured by a scene in the movie ‘As Good As It Gets’ when actress Helen Hunt weighed in on her ‘piece of sh*t HMO‘ denying her access to covered services. As I recall, the entire audience laughed identifying with her animus towards HMOs.
This moment in popular culture represented the public’s push back to ‘gatekeeper model‘ HMOs where primary care physicians ran interference between a member and his or her referral to a specialist consult or hospital admission.
To meet rising consumer frustration and the employer sponsors the plans growing concerns. right around this time (circa mid to late 90s), United Healthcare introduced PPO plans and ‘direct access’ HMO versions as well that permitted specialist referrals without the consent of the primary care gatekeeper.
What soon followed was an era of risk push-back particularly as more consumers rebelled against gatekeeper HMOs, and a lot of red ink for risk bearing IPAs, medical groups or even PHOs (physician/hospital organizations) who took on health plan risk, incurring massive operating losses. While premium increases were restrained to declining, the per member per month (PMPM) or percentage of premium contract dollars passed to participating risk bearing providers represented declining baselines for payment of covered services.
Back to the Future: ‘Deja Vu’ Again?
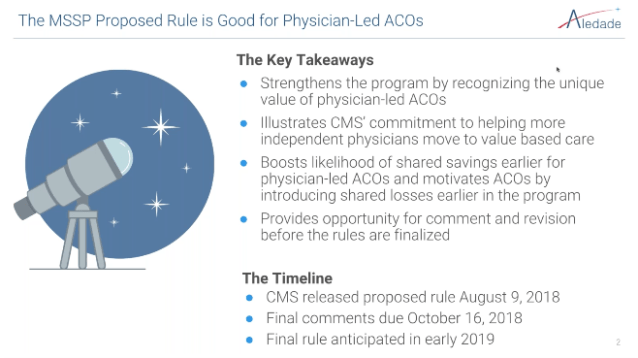
With the passage of the Affordable Care Act (ACA) principally designed to increase access, reduce the rate of uninsured Americans’ and lay the seeds of cost containment innovation principally via Accountable Care Organizations (ACOs) – the majority participating in upside gain share only in the Medicare Shared Savings Program (MSSP) – but also encouraging pilots and demonstration efforts at the Center for Medicare and Medicaid Innovation (CMMI) we’ve re-entered another era of measured risk transfer 2.0 with the provider community (i.e., hospitals, physicians and allied health practitioners).
As the principal workhorse in the ‘innovation lab‘, six years in ACOs have been a net disappointment in terms of producing the expected savings – though their quality performance metrics are a different story – initially envisioned leading up to the law’s passage. Yet amidst contentious and shifting sands of both federal and state health policy guidance in the transition from the Obama to the Trump administration, one goal remains intact with seemingly solid bi-partisan support: the continued investment in and active pursuit of a value based (vs. production fueled fee-for-services) healthcare economy. Whether via top down federal policy or the granular baking of innovation from the grassroots up, we’ve returned to the drawing board of finding a delivery and financing system that can deliver on the promise of the triple aim – better care, better outcomes at lower per capita costs.
Enter Direct Primary Care aka ‘DPC’
In 1913 Dr. Charles Mayo one of the three founding brothers of the Mayo Clinic weighed in rather optimistically on the future of medicine delivered primary via seamless, team based healthcare. Yet, some 100 plus years later, are we there yet? I think the answer is a resounding no. But why the glacial pace of progress in a seemingly transformation resistant healthcare industry?
 With layers of failed generational innovation and the inherent complexity grafted on each wave of the transformational impulse, we as an industry of stakeholders writ large (i.e., hospitals, physicians, regulators, payors, brokers, underwriters, investors and a litany of too numerous to mention suppliers and vendors at the trough) have co-created an incoherent, inefficient, costly and burdensome ‘provider centric’ healthcare economy with conflicted incentives, and little to no alignment with the mission towards building a quality, affordable healthcare economy that works for us al
With layers of failed generational innovation and the inherent complexity grafted on each wave of the transformational impulse, we as an industry of stakeholders writ large (i.e., hospitals, physicians, regulators, payors, brokers, underwriters, investors and a litany of too numerous to mention suppliers and vendors at the trough) have co-created an incoherent, inefficient, costly and burdensome ‘provider centric’ healthcare economy with conflicted incentives, and little to no alignment with the mission towards building a quality, affordable healthcare economy that works for us al
In 2018 this de-facto ‘non-system‘ aggregate is at risk of imploding on itself. No-one is happy. From frustrated patients, to disillusioned clinicians, to disaffected employers and a somewhat drifting [see: ‘Rethinking The Physician-Focused Payment Model Technical Advisory Committee (PTAC)’ which addresses the ‘rising tensions’ between PTAC, and HHS] federal government are all scrambling to find solutions that deliver value.
A novel model launched in the late 90s by Garrison Bliss, MD introduced ‘direct primary care‘ (DPC) initially via Seattle Medical Associates which then re-tooled into the Qliance brand. Qliance created a fair amount of buzz and spawned considerable competition while advancing the standing of DPC. Yet, a ten year run promptly came to an end when Qliance ceased operations in June of 2017.
 Dr Bliss’s legacy contributions live on as he cleared the path for DPC in the state of Washington via enabling statute. DPCs are required to register and report annually (2017 report, here) to the Department of Insurance (definition of DPC, here) a basic data set including: fees charged, enrollment, participating physicians and practice locations. He also presided over the inclusion of DPCs in Qualified Health Plan offerings listed on ACA exchanges. See below:
Dr Bliss’s legacy contributions live on as he cleared the path for DPC in the state of Washington via enabling statute. DPCs are required to register and report annually (2017 report, here) to the Department of Insurance (definition of DPC, here) a basic data set including: fees charged, enrollment, participating physicians and practice locations. He also presided over the inclusion of DPCs in Qualified Health Plan offerings listed on ACA exchanges. See below:
Treatment of Direct Primary Care Medical Home, 76 Fed. Reg. 41900 (July 15, 2011) (amending section 1301(a)(3) of the Affordable Care Act)
A “Direct Primary Care Medical Home” plan is defined as “an arrangement where a fee is paid by an individual, or on behalf of an individual, directly to a medical home for primary care services, consistent with the program established in Washington.” (Federal Register Citation)
Meanwhile, the data since reporting began in 2007 is instructive on the limited appeal and slow uptake to date of the DPC model in the population at large, and in my view represents a bellwether for the rest of the nation, see HintHealth 2017 survey here, further documenting the very limited penetration of DPCs into the mainstream market.
Thus, Washington state became the first state to define and regulate direct primary care practices and to prohibit direct practice providers from billing insurance companies for services provided to patients under direct practice agreements.
- Ten years later, DPC enrollment totaled 14,790 direct practice patients out of 6.7 million Washington state residents, a 0.22 percent share of the population
- Overall patient participation increased 31%, from the fiscal year 2016 total of 11, 272 participants to 14,790 (an increase of 3,518 participants)
Under the Hood of a DPC: Is it ‘HMO Lite’?
First up, let’s examine one definition proffered by a visionary DPC advocate and practitioner who is also a practicing attorney, Phil Eskew, DO, JD:
For the practice to qualify as a direct primary care practice, the practice must:
- Charge a periodic fee
- Not bill any third parties on a fee for services basis; and
- Any per visit charge must be less than the monthly equivalent of the periodic fee
At it’s core a DPC looks like and to some degree models a ‘lite’ version of a PCP gatekeeper HMO. This includes monthly global prepayment, a defined set of covered services, an assigned patient (member) panel (albeit considerably smaller than a participating PCP in an HMO), and since compensation is budget driven and prospectively paid – little if any of the billing and coding complexity associated with the traditional billing and collections model of FFS based PCP practices.
Unlike an HMO a DPC is not a risk bearing concern other than the sponsoring physicians who go at risk for their professional services. In fact most DPCs are strongly encouraged to operate in a safe harbor of what might otherwise be deemed to be operating in the business of insurance as unlicensed and thus illegal entity.
While not a risk bearing operation per se, DPC models operate in the wild west, where if you’ve seen one practice’s footprint, you’ve seen one DPC operation. There are no standards and there are no compare and contrast opportunities. DPCs are in no way a homogeneous group, rather they are the byproduct of a patchwork of state laws, and the goals, competencies and intentions of the owner physicians.
DPCs must refer out all hospitalizations, outpatient surgeries, costly imaging or lab testing, and specialist consults, etc. Thus DPC practices will optimally work only when layered into ‘wrap around’, catastrophic or prevailing high deductible or rebranded ‘consumer directed’ health plans – though some DPC models, i.e., My MD Connect and others, are designing products for brokers and stop loss carriers offering health plan options for self insured employers built on a network of participating DPC practices.
Some DPCs will negotiate with select preferred specialists, routine lab testing and for certain imaging services. But each practice will have a different menu of primary care services and what may be included in referred care.
Market Results
In a recently published article at the Journal fo the American Board of Family Medicine titled: Direct Primary Care: Applying Theory to Potential Changes in Delivery and Outcomes, the author concludes as follows [emphasis bolded mine]:
The need for rigorous research on the DPC model is great. The American College of Physicians has made such a call, beginning with the most basic descriptive patient and provider variables.41 Information on participating patient demographics before and after DPC adoption is required to understand the population that is served by DPC and the broader implications for excluded patients. Research on the patterns of DPC location and socioeconomic context would also provide a better understanding of DPC’s niche. Following these descriptive analyses, the focus must shift toward outcomes and the attainment of the 4 attributes of primary care, with comparisons between DPCs and other models of primary care. Although this research will encounter obstacles, such as the absence of claims data for DPC practices, it is essential to guide providers, patients, and policy makers toward high-quality primary care.
Meanwhile, theoretic application informed by years of research on primary care provides insight as to what changes to expect and to monitor as practices consider DPC adoption. By applying Starfield’s conceptual model, an understanding of the potential changes to structures, processes, and outcomes for the patient population can be achieved while policy makers and providers await rigorous research on DPC. Evidence exists to support DPC as a theoretically sound approach to attaining the attributes of first contact care and longitudinality for participating patients. DPC uses changes to financing and the population eligible to trigger these potential improvements. At the health system level, DPC has low-construct validity to support a positive impact on the potentially eligible population. By limiting access to those willing and able to pay the membership fee, a vulnerable population will almost certainly be excluded. A model that does not meet the needs of a vulnerable population is unlikely to have a significant impact on the overall costs and outcomes of the US health care system. Other policies and models to address primary care financing and accessibility that do not exclude groups of patients exist and may or may not be superior to DPC. DPC’s distinguishing characteristic from these other models is that the control rests with the PCP and is not dependent on financing from third-party payers.
Complete article: Direct Primary Care: Applying Theory to Potential Changes in Delivery and Outcomes
The Road Ahead
For DPCs to scale and make a systemic impact beyond the local community in which their owners/sponsors operate and become more than a lifestyle, ethical decision or political statement giving the finger to ‘the man’, they’ll need to somehow get their arms around ‘downstream’ network risk and define certain minimum operating requirements or standards which apply to all DPCs equally.
Though therein lies part of the problem. The safe harbor contours mentioned earlier is not iron clad and is more or less protected by variable states statutes exempting DPCs from being in the business of insurance. Any argument that can validly be made that the DPC is assuming ‘risk’ beyond the primary care services in the contract between the DPC practice and its members is one more arrow in the quiver of state department of insurance commissioners’ tasked with the protection of patients purchasing health insurance.
Two groups have organized to harmonize and advance the practice of DPC including the Direct Primary Care Coalition and DPC Alliance, the former chaired by Garrison Bliss, MD (see leadership here) and the latter Ryan Neuhofel, DO, MPH. Both proactive and visionary physician leaders committed to supporting and leveraging the business model of DPC given the heterogeneity of its member practices.
ACO and DPC Synergies?
While I do not have a business plan or model for a hybrid version or combination ACO/DPC derivative, it seems a venn diagram can identify characteristics common to both operating footprints mentioned above. Since we’re all still looking for ways to tame the rapacious appetite of a seemingly insatiable and predominantly fee-for-services fueled healthcare delivery and financing ecosystem, what do we have to lose?
Let’s think out of the box! We can do this!






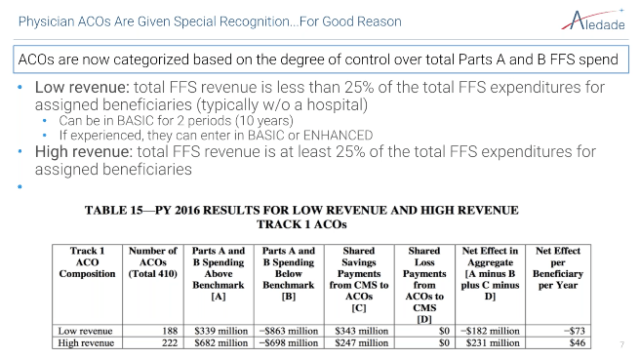




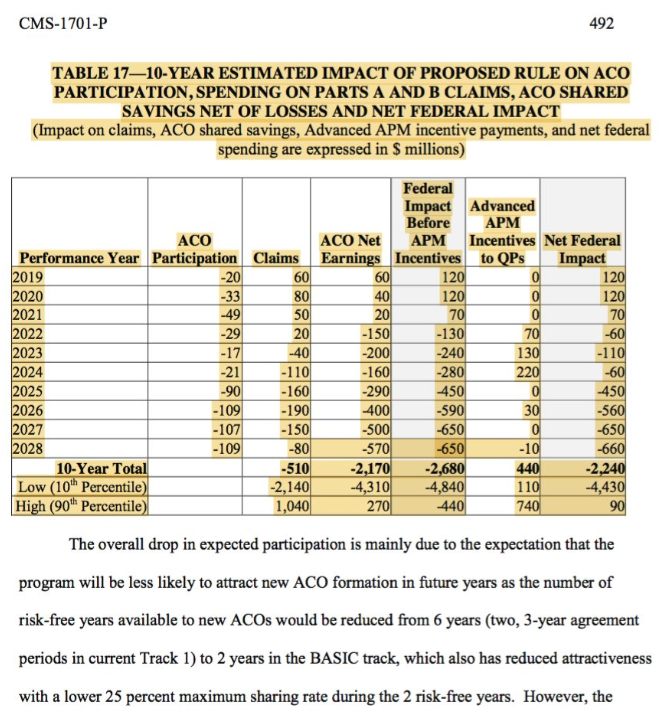
 9/ But what this initial release does not help us do is see which type of ACOs are creating the most value. My guess is that it’s not much different from what the CMS actuaries found for PY 2016 – ACOs that include hospitals and directly control more of the cost of care do worse.
9/ But what this initial release does not help us do is see which type of ACOs are creating the most value. My guess is that it’s not much different from what the CMS actuaries found for PY 2016 – ACOs that include hospitals and directly control more of the cost of care do worse.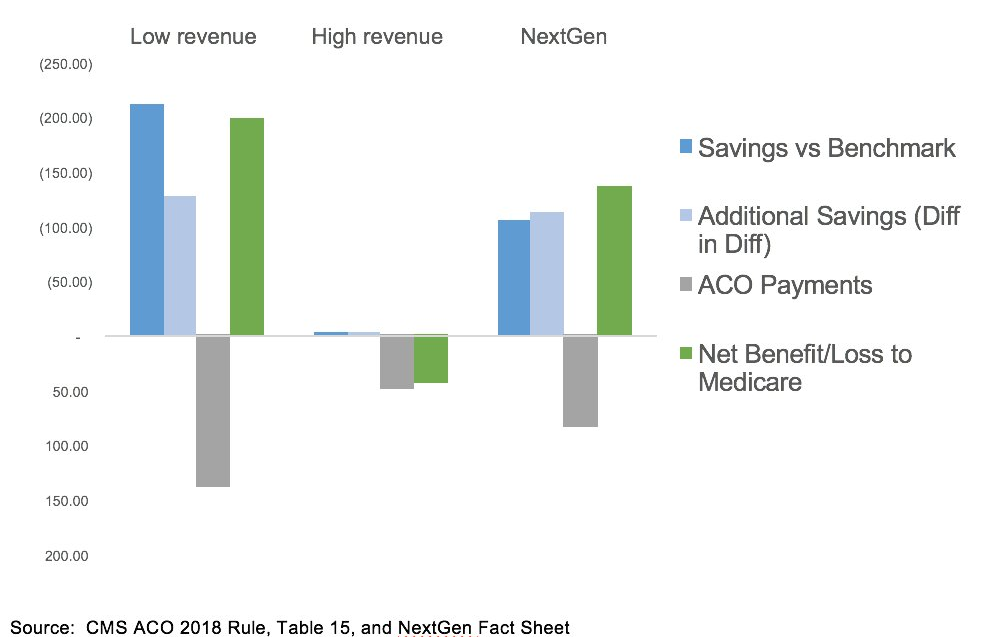 10/ The “low revenue” ACOs (in the OACT analysis – less than 10% of total cost of care came to them) were only a third of the lives in the program, but generated roughly 98% of the savings. THAT is why in the ACO Rule CMS proposed letting them stay in low risk models longer.
10/ The “low revenue” ACOs (in the OACT analysis – less than 10% of total cost of care came to them) were only a third of the lives in the program, but generated roughly 98% of the savings. THAT is why in the ACO Rule CMS proposed letting them stay in low risk models longer.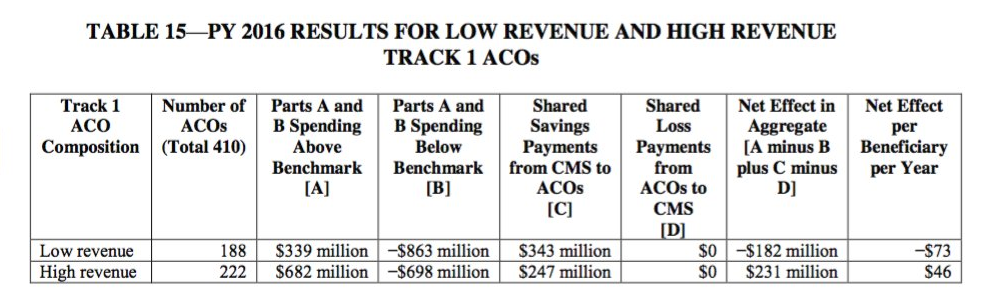 11/ That was the entire thesis behind “the paradox of primary care leadership” that informed the founding of
11/ That was the entire thesis behind “the paradox of primary care leadership” that informed the founding of