
by Gregg Anthony Masters, MPH & Fred Goldstein, MS **
PopHealth Week | Healthcare NOW Radio Host: Fred Goldstein, President, Accountable Health, LLC Executive Producer & Co-Host: Gregg Anthony Masters, MPH Episode Theme: “Enough Is Enough” – The Decimation of Public Health Infrastructure, the Rise of Health Quackery, and Why Science Still Matters
“Silence is acceptance people. Speak up!” – Gregg Anthony Masters, MPH, closing the episode
Introduction: When Professionals Say Enough
There comes a moment, sometimes quiet, sometimes explosive, when a person who has spent decades navigating institutions, absorbing dysfunction of ‘managing’ complex enterprises whether health plans or health systems, and advocating for incremental reform simply decides: no more. That moment arrived for Fred Goldstein, President of Accountable Health, LLC, and a recognized voice in population health, managed care, and evidence-based healthcare delivery.
On this episode of PopHealth Week, Fred once again stepped into the guest SME (subject matter expert) chair to unpack the essays he published on his PopHealth Pulse and LinkedIn under a title that said everything: “Enough is enough” and “People, Health, Research and Reality”.
His executive producer and co-host for the day, Gregg Anthony Masters, MPH, framed the conversation squarely and without ceremony: this was about the systematic dismantling of public health infrastructure, the ‘weapon-ization’ of social media against scientific literacy, and the long-unresolved contradiction at the heart of American healthcare – a system that was never really designed to produce health.
What followed was one of the most direct, experience-grounded conversations in the show’s run. No hedging. No false balance. Just two seasoned public health professionals, credentialed and candid, saying what the data and their careers have confirmed.
Part I: What “Public Health Infrastructure” Actually Means
One of Gregg’s most clarifying moves was to refuse the narrow definition of public health infrastructure and insist on the broader one. In popular discourse, “public health” often conjures health departments, ie, chronically underfunded agencies staffed by mission-driven clinicians who, as he put it, had to be “heart centered” to choose that career path “because the money ain’t there.”
But Fred and Gregg broadened the frame deliberately: legacy public health infrastructure (underfunded, often understaffed, overworked health departments, poorly synced with acute health care assets – think the ineffective handoff of Ebola cases in Dallas circa 2014) includes CMS, Medicare, Medicaid, and the full architecture of Title (XIX & XX) programs that fund and structure American healthcare delivery. It includes the research enterprise at NIH and the critical international disease surveillance network anchored by USAID. It includes housing policy, clean water, education, and the social determinants of health that account, by most estimates, for 80 percent or more of health outcomes.
This is not a rhetorical expansion. It is epidemiologically accurate. The World Health Organization defines social determinants of health (WHO) as the conditions in which people are born, grow, live, work, and age, coupled with decades of research confirm that income, housing stability, educational attainment, and neighborhood safety drive health outcomes more powerfully than any clinical intervention. When you defund housing programs, you are defunding health. When you eliminate food assistance, you are eliminating a health intervention. The infrastructure is one system, even if it is administered across dozens of agencies.
Fred named the pattern plainly: “what is being cut is not bureaucratic waste. It is the scaffolding that keeps people alive.”
Part II: DOGE, USAID, and the Epidemiological Consequences of Dismantling Global Surveillance
The conversation turned to one of the most consequential policy decisions in recent memory: the near-total dismantling of the United States Agency for International Development (USAID). Fred and Gregg cited this as one of the worst offenses in the broader campaign of senseless institutional destruction of modest public health interventions with a very high ‘return’ to the community.
USAID’s public health programs were not primarily charity. They were strategic. The agency maintained disease surveillance networks across dozens of countries, funded outbreak response capacity, and supported the kind of early-warning infrastructure that gives health systems time to respond before a pathogen becomes a pandemic. PEPFAR, administered through USAID, has saved an estimated 26 million lives since its 2003 launch. USAID’s tuberculosis programs treat millions annually in countries where, without treatment, extensively drug-resistant strains develop and spread – including, eventually, to the United States.
Fred stated the logic simply: we are interconnected. Pathogens do not respect borders or visa requirements. “Someone comes across on a cruise or a boat,” he said or, as the COVID-19 pandemic demonstrated, on a plane connecting through a major international hub. The current Ebola outbreak in the Democratic Republic of Congo was offered as a live example: the same kind of outbreak USAID was built to monitor and contain at the source.
Investments in disease management vs. public health infrastructure
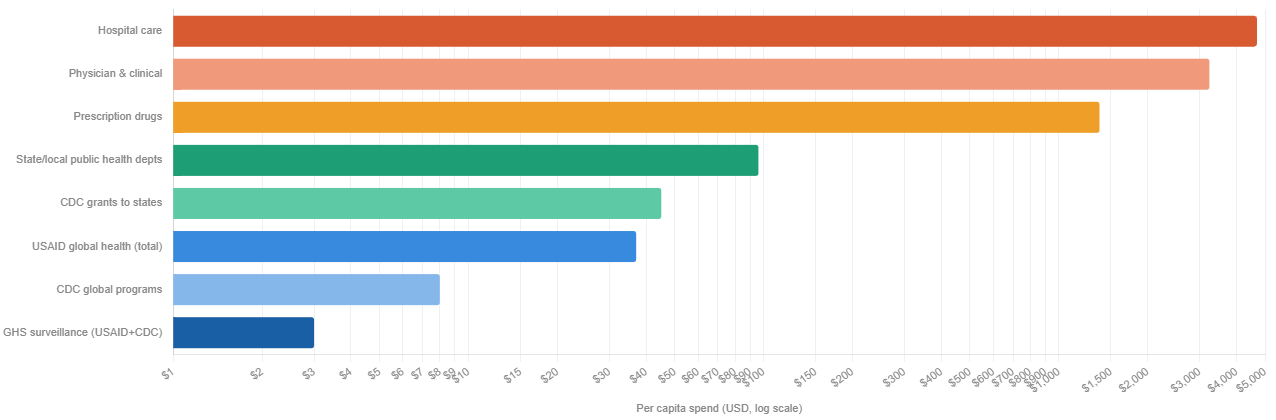
- Ratio: hospital care vs. global surveillance 565:1
- per dollar spent on global health security (GHS) programs
- Public health as share of total spend
- all prevention combined, per TFAH
- COVID economic cost vs. 5-yr GHS spend
- $14T loss vs. $1B prevention investment
Sources: CMS National Health Expenditure Accounts 2024; KFF; Trust for America’s Health; GAO; Johns Hopkins Center for Health Security. US population ~335M used for per capita calculations. CDC global programs ~$700M; GHS combined USAID+CDC ~$993M (FY2025 CR level). State/local public health includes federal grants to states.
The Centers for Disease Control’s Global Disease Detection program, which partnered closely with USAID, exists precisely because the cost of surveillance is a fraction of the cost of pandemic response. A 2019 report by the Johns Hopkins Bloomberg School of Public Health estimated that a severe respiratory pandemic could cost the global economy $570 billion annually. Defunding the early-warning systems that prevent such events is not fiscal prudence. It is a catastrophic risk transfer from the present to the future.
Part III: NIH Cuts and the Strategic Suicide of Defunding Research
Fred’s frustration was palpable when the conversation turned to NIH funding cuts. “The idea of cutting these NIH funds around research is just bonkers,” he said. “This country has been amazingly great and built upon the power of research.”
This is not nostalgia. It is economics. The National Institutes of Health funds research that has produced more pharmaceutical breakthroughs, more diagnostic innovations, and more clinical protocols than any comparable institution on earth. A United for Medical Research (UMR) 2026 Report: “NIH’s Role in Sustaining the U.S. Economy FY 2025” analysis found that every federal dollar invested in NIH research generates roughly $2.57 in economic activity. The mRNA technology underlying COVID-19 vaccines, developed with substantial NIH funding over decades, saved millions of lives and demonstrated that basic research investment has compounding returns that are impossible to predict in advance but catastrophic to forgo.
Fred invoked the HIV/AIDS research arc as the definitive case study in scientific iteration. From the first clinical descriptions of a mysterious immunodeficiency syndrome in 1981 to the identification of HIV, the development of AZT, the breakthrough of triple-combination antiretroviral therapy, the elucidation of viral load and CD4 counts as clinical markers, and the current era of PrEP, which can reduce the risk of getting HIV acquisition risk by as much as 99 percent in those who take it consistently – the arc took four decades of funded, iterative, sometimes-wrong-but-self-correcting science. None of it would have happened without sustained public investment.
“You never know what’s going to come out of some research project,” Fred noted. “It may lead to another great discovery.” This is not a platitude. It is the documented history of penicillin, of the polio vaccine, of chemotherapy, of statins. Defunding research does not eliminate need. It eliminates the capacity to meet it.
Part IV: The Scientific Literacy Crisis – How We Got Here and Why It Matters
Perhaps the most sobering section of the conversation addressed why false health claims spread so much faster than evidence. Fred and Gregg identified a convergence of forces:
1. Education gaps around scientific process. Most Americans never learn what science actually is, an iterative, self-correcting methodology that moves, as Gregg put it, “from unreasonable certainty to reasonable uncertainty.” Science does not produce Truth with a capital “T” on first contact. It produces provisional, probability-weighted conclusions that grow stronger with replication. That is not a weakness. That is the mechanism. But to someone who has never been taught how science works, the iterative nature looks like inconsistency, and inconsistency looks like unreliability.
2. Abbreviated attention spans. Fred cited an observation from a film school that younger students are struggling to sit through feature-length films because short-form social media content has restructured their attention patterns. The American Psychological Association (APA)has documented the relationship between heavy social media use and reduced capacity for sustained attention. Short-form claims, delivered with confidence, are cognitively easier to process than qualified, data-heavy arguments. Misinformation is almost always shorter than the truth.
3. The amplification of confident wrong voices. Fred described listening to a social media personality with millions of followers making claims he found “completely crazy.” His sons listened for ‘entertainment’. Millions listened for ‘guidance’. The Reuters Institute Digital News Report has consistently found that significant portions of the public receive health and science information through social media, often from sources with no relevant credentials.
4. The supplement and wellness industry’s exploitation of regulatory gaps. The Dietary Supplement Health and Education Act of 1994 created a framework in which supplement manufacturers bear no pre-market burden to demonstrate efficacy or safety. Claims that products “support” various functions proliferate without double-blind trials. Fred identified this as a deliberate exploitation of public scientific illiteracy and named it accurately as ‘health quackery’, given new life by a policy environment that values bold declarations over peer review.
Part V: The ADA Conference Incident – When Institutions Suppress Dissent
One of the episode’s most striking moments came when Fred described a scene at the American Diabetes Association’s recent scientific conference: researchers who had published an editorial in the ADA’s own journal, concerning NIH cuts and research funding, were handing out copies of that published work at the conference. They were escorted out by police!
This deserves to sit with you for a moment. A peer-reviewed article. In the associations own journal. Distributed at the association’s own conference. And the authors were removed by law enforcement.
Fred noted that subsequent resignations from the ADA followed. Gregg named the dynamic without euphemism: “there is a chill”. Professional associations that depend on relationships with federal funders, on conference sponsorships, and on not provoking regulatory scrutiny are making institutional calculations that silence their own members.
This is not unprecedented. Research on self-censorship in scientific communities has documented the ways in which funding dependencies, career pressures, and fear of political backlash suppress scientific speech, particularly on contested policy questions. What is notable is how openly it is now happening, and how quickly institutions that existed to advance scientific knowledge are retreating from that mission when it becomes inconvenient.
Part VI: The Broken Healthcare System: A Disease That Predates DOGE
Both Fred and Gregg were careful to separate two problems that are related but distinct:
Problem One: The current administration’s cuts to research, public health infrastructure, and social support programs. This is acute damage being done in real time.
Problem Two: The structural failure of the American healthcare delivery and financing system. This is chronic. It predates the current political moment by decades.
Gregg has tracked the evolution of this system with the granular attention of someone who has lived inside it. He walked through the arc: HMOs, then IPA spin-offs, followed by PPOs (which were more “palatable” to the group health market that didn’t want narrow networks), the ACA (Affordable Care Act) introduced ACOs, value-based care organizations, and corporate managed care organizations in various iterations. None of them, he noted, have solved the fundamental problem. They have created “more hurdles and obstacles for people to jump through to get needed care.”
Meanwhile: costs continue to accelerate driving widespread affordability claims as more and more of the liability shifts from plan to member via increased premiums, copays, coinsurance and deductibles due in large part due to the failure of House and Senate Republicans to extend ACA premium tax credits (subsidies). Meanwhile, access remains spotty. And quality is, in Gregg’s word, “a crapshoot.”
Gregg referenced a colleague’s new book “Healing the Sick Care System and Why Patients Matter” by Gil Bashe, which argues that the healthcare system views itself as the client, not patients. Fred agreed with the diagnosis but offered a defense of physicians: most clinicians entered medicine to help. The system does not allow them to. If a primary care physician in a fee-for-service environment keeps a patient healthy, that physician makes less money. A healthy patient generates no revenue. As Gregg further articulated: “There is no prevention business model as long as you run on a fee-for-service chassis.”
This is a structural incentive problem, not a character problem. And it is one that decades of health economics research has confirmed. Fee-for-service payment rewards volume and complexity. It penalizes efficiency and prevention. Value-based care models have attempted to reorient incentives, but Fred cited research suggesting the results have been modest at best – bending a 4 percent cost trend to 3.5 percent is not the systemic transformation advocates hoped for. The system, as he put it, “will not let” costs actually drop.
The brutal arithmetic of insurance: a health plan that successfully keeps its population healthy will collect premiums on a healthier pool, generate fewer claims, and in the ACA (Affordable Care Act) medical loss ratio framework find itself returning money if its loss ratio drops too low. The financial incentive structure does not reward health. It rewards the management of illness at a profitable margin.
Part VII: Physician Burnout as a System Failure, Not a Personal Failure
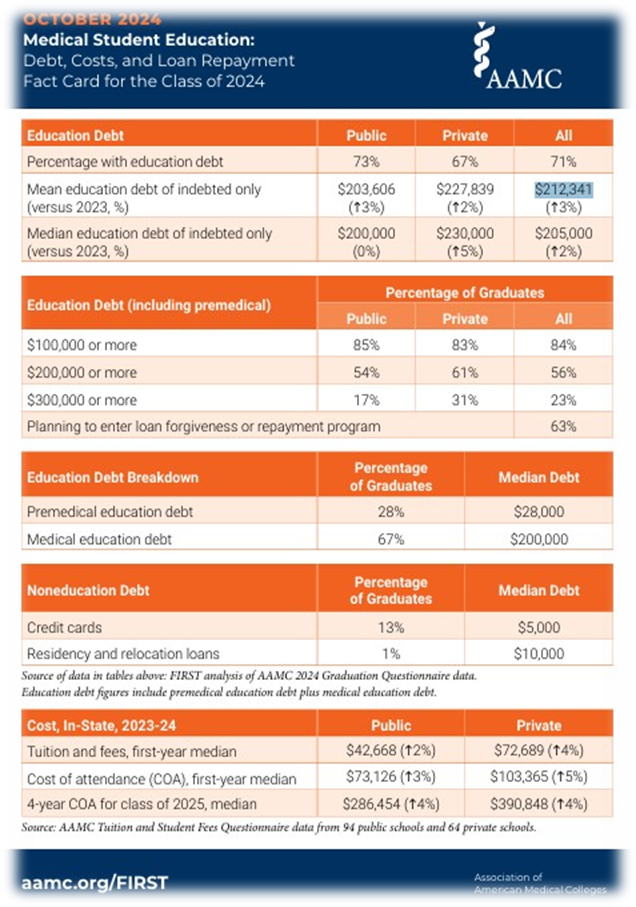
Gregg raised what he described as the ‘brain drain’ waste embedded in physician training coupled with growing exits to entrepreneurial or other administrative roles, ie, CMIOs. The public investment in producing a physician – four years of undergraduate education, four years of medical school, three to five years of residency, often additional fellowship training – represents up to a sixteen years of intensive investment, plus a debt load that for many physicians (public and private) averaged $212,341 according to Association of American Medical Colleges (AAMC) Medical Student Education: “Medical Student Education: Debt, Costs, and Loan Repayment Fact Card for the Class of 2024 “.
When those physicians burn out and exit clinical practice, opting for administrative roles, i.e., CMO (chief medical officer) and other positions, entrepreneurial ventures, or simply early retirement, the human capital loss is staggering.
The root cause is not individual weakness. It is system design. Dr. Tait Shanafelt, professor of medicine and chief wellness officer at Stanford Medicine, describing the cultural mindset that long prevailed:
“There was this rite of passage mindset of: I went through it, it was formative – you should go through it too.”
Further, AMA research on physician burnout has documented the relationship between administrative burden, moral injury (being unable to provide care one knows is necessary), and the psychological costs of navigating prior authorization, documentation requirements, and corporate ownership pressures. When physicians are acquired by hospital systems or venture capital firms, clinical autonomy often diminishes. “They ain’t gonna let you do that,” Fred said, referring to the practice of prioritizing patient health over admissions and procedures.
The result is a primary care desert at precisely the moment primary care is most needed. Fred’s point was unambiguous: if you want to improve population health, you need more primary care access. You need more physicians oriented toward prevention, continuity, and the whole patient.
And ‘the system’ as currently designed actively discourages that.
==##==
** AI Use & Editorial Standards Disclosure. In producing this content, the authors employ AI language tools in a defined supporting role: (1) Research aggregation: surfacing relevant source material and authoritative references across peer-reviewed, institutional, the arts and journalistic databases; (2) Structural organization: proposing content architecture and draft sequencing; (3) Draft suggestion: generating candidate language for author review. The authors retain sole editorial responsibility for all published content. Every citation is independently confirmed as accurate and accessible prior to publication. No headlines, pull quotes, or factual claims are published without author verification. AI-generated language is treated as raw material then recast entirely in the authors’ established voices and subject-matter expertise before any content reaches publication. This workflow reflects the authors’ commitment to the standard that AI serve, not replace the author.
