
Part I: Leadership Isn’t the Problem. Leadership Is the Symptom.
By Gregg Anthony Masters, MPH**
Today I read a piece quoting the insights of Sachin H. Jain, MD, MBA, FACP, CEO of SCAN Group, SCAN Health Plan, and Forbes contributor, titled: “Healthcare’s problem isn’t the system, it’s us”.
The core argument:
- The “it’s us“ indictment. In each of his three decades in healthcare, Jain has faced a different “boogeyman,” from the quality crisis to coverage expansion to today’s push toward value-based care. Each time, the industry implemented a fix, yet nothing improved. His conclusion: “It’s us. We’re not necessarily taking charge of the problems that are under our control.”
- Toxic positivity as strategic evasion. Rather than acknowledging the real anger over cost, denials, and administrative burden, executives simply pointed to the flawed system. Jain’s view: “You can’t fix something until you actually acknowledge it’s a problem.” He concluded bluntly: “No one’s buying it anymore.”
- The “no margin, no mission” trap. Jain cited a cardiologist at a Northeast academic medical center who built a heart failure program keeping patients out of the hospital. The hospital’s response was to ask what the department was doing wrong since admissions had dropped. When the physician explained the program was working, he was told: “No margin, no mission.” Jain argued this phrase has become a cover for exactly the kind of leadership failure he was describing.
- Latent leadership capacity being killed. “We have so much more latent leadership capacity in this industry than we’re exercising. We have so many people with so much ingenuity, creativity, drive and passion, and we kill it.” His prescription: the number one way to improve healthcare is to tap leaders who genuinely support and desire an improved system.
- Courageous challenge as organizational culture. At SCAN, Jain has made “courageous challenge” a core organizational value, giving employees explicit permission to stand up and say something that goes against the grain, creating an environment where difficult conversations and hard questions are not just tolerated but encouraged.
- Accountability means being reachable. Every quarter, Jain sends his personal work email to each of SCAN’s 440,000 members and reads three types of messages daily: one from a satisfied member, one offering helpful advice, one who is angry. His view: “We hide behind HIPAA, we hide behind the ACA, we hide behind whatever rules we think we can hide behind.” vaticahealth
- Depth over breadth, “monogamy” in provider-plan relationships. Jain argued healthcare is “extraordinarily promiscuous,” with providers partnering with every plan and plans partnering with every provider group. No one builds anything deep enough to change the patient experience. He pointed to SCAN’s strategy of asking provider partners to stop splitting membership across every plan and work with SCAN exclusively, asking what it would look like to have a shared call center, a shared patient record, and shared accountability for outcomes.
This ‘fireside chat’ triggered and prompted reflection on his argument and the need to reply via a series of posts to this audience.
Every generation of healthcare executives believes it has inherited a uniquely broken system.
It hasn’t.
American healthcare has been declared “unsustainable” almost continuously since Medicare and Medicaid were enacted in 1965. Costs have risen. Technology has advanced. Institutions have consolidated. Payment models have evolved from indemnity insurance to HMOs, PPOs, ACOs, bundled payments, Medicare Advantage, Direct Contracting, ACO REACH, and now artificial intelligence-enabled utilization management.
Yet one uncomfortable fact remains. The underlying economics have changed remarkably little.
That is why Sachin Jain’s recent essay, Healthcare’s Problem Isn’t the System – It’s Us, deserves attention. His central argument is provocative precisely because it rejects one of healthcare’s favorite excuses, i.e., that “the system” (aka the @HealthcareBorg) is somehow responsible for our collective inability to transform care and optimize outcomes.
He argues instead that healthcare’s greatest obstacle is leadership. Executives normalize dysfunction, defer difficult decisions, and hide behind complexity instead of exercising moral courage. It is a compelling critique because it contains more than a grain of truth.
Indeed, leadership matters. Organizations do not transform themselves. People do. But I would suggest Jain’s diagnosis stops one layer too soon:
- Leadership is not the disease.
- Leadership (or some may say absence of) is the symptom.
The disease is an incentive structure that rewards institutional preservation over institutional transformation.
That distinction matters because it explains why otherwise capable leaders repeatedly make decisions that appear timid, contradictory, or strategically incoherent.
We Don’t Have a Leadership Crisis
Contrary to popular opinion, American healthcare does not suffer from a shortage of intelligent executives. Quite the opposite.
Healthcare is populated by extraordinarily talented physicians, administrators, economists, data scientists, entrepreneurs, operators and yes, even actuaries. Few industries possess comparable intellectual capital.
Nor is there a shortage of strategic plans. Every health system now speaks fluent “value.” Every payer proclaims patient-centeredness. Every annual report celebrates innovation. Every conference keynote extols digital transformation. Every strategic retreat promises to “meet patients where they are.”
And yet fee-for-service continues to dominate organizational behavior. Not because executives secretly oppose value-based care. Because they are compensated to preserve existing revenue streams while cautiously experimenting around the edges.
That isn’t cowardice. It’s governance.
Boards hire CEOs to protect enterprise value.
- Bond ratings.
- Operating margins.
- Market share.
- Debt covenants.
- Credit access.
- Political relationships.
- Employment stability.
The healthcare CEO who voluntarily cannibalizes profitable fee-for-service revenue in pursuit of uncertain long-term value may be admired by academics. Yet, he or she is far less likely to survive the next compensation committee meeting.
Leadership, in other words, operates within constraints that are rarely acknowledged in popular discussions about healthcare transformation.
Culture Doesn’t Create Incentives
Healthcare management literature frequently asserts that “culture eats strategy for breakfast.” The aphorism has become management orthodoxy. But in healthcare, incentives generally eat culture. Yet, truth is ‘culture’ follows payment. One need only observe how quickly provider behavior changes when reimbursement changes:
- Hospital admissions.
- Observation status.
- Readmission penalties.
- Risk coding.
- Quality reporting.
- Telehealth.
- Hospital-at-home.
- Every one of these evolved not because organizational culture suddenly matured but because financial incentives shifted.
- Executives responded rationally.
As they should. This is not a moral failure. It is economics, full stop. Healthcare organizations are adaptive organisms. They evolve toward reimbursement, often quoting ‘no margin, no mission’.
The Myth of “The System“
Ironically, I agree with Jain on one point. Healthcare leaders often invoke “the system” as though it were weather. Immutable. Uncontrollable. An external force beyond human agency. But systems are not acts of nature. They are collections of incentives designed and continually redesigned by policymakers, regulators, employers, insurers, providers, investors, and consumers. The system behaves exactly as it has been designed to behave. Its outcomes may be undesirable. They are rarely accidental.
The ‘Missing’ Conversation
What remains surprisingly absent from contemporary healthcare leadership discussions is political economy, i.e., you can’t implement policy absent the enabling politics of ‘winning’ elections. Healthcare does not merely allocate clinical resources. It allocates financial power (minimally think proceduralist vs cognitive biases). Every reform proposal creates winners and losers. Every payment redesign redistributes income. Every consolidation shifts bargaining leverage. Every new benefit changes market share. Leadership, to the extent it can be ‘homogenized’ into best practices, alone cannot overcome those structural realities. Nor should we expect it to.
A Generation of ‘Deferred’ Decisions
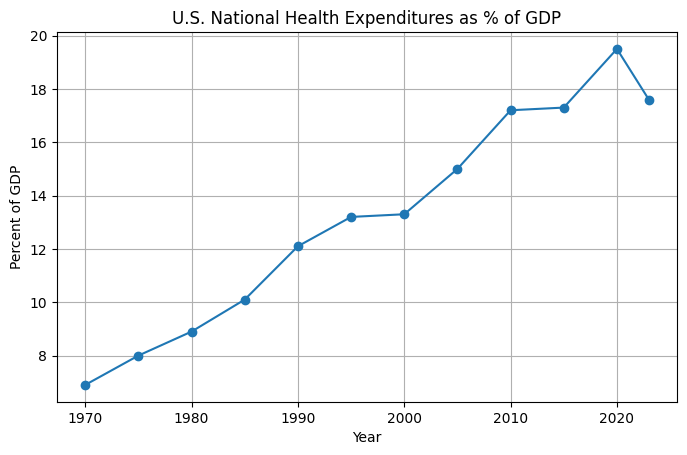
The irony is both persistent and painful. The healthcare industry has spent nearly forty years ‘discussing’ transformation. When I started the GDP of healthcare share was 8-9 % range, today it’s just shy of 20%.
Secular themes, you know the organizing value proposition of push/pull industry top lines at major healthcare innovation conferences from HiMSS to HLTH with many in between including Health Datapalooza, JP Morgan Investor Healthcare Conference, NextMed (formerly Exponential Medicine and FutureMed, etc.) popularly engage:
- Disease management.
- Managed competition.
- Integrated delivery.
- Consumer-directed care.
- Medical homes.
- Population health.
- Accountable Care Organizations.
- Precision medicine.
- Digital health.
- Artificial intelligence.
Each promised structural change. Most produced incremental adaptation where one-off or niche (think Dave Chase and Rosetta innovation for self-funded employer sponsored health plans) vs. ‘systemic’ relief, i.e., advancing the triple let alone more ambitious ‘quadruple’ aim of clinician work/life satisfaction.
Why?
Because almost every reform was layered on a chassis of existing fee-for-service economics rather than replacing them. We reflexively create hybrid systems instead of new systems. Organizations therefore learned to optimize for both worlds simultaneously. Volume finances value. In turn value justified volume. Everyone learned the language and adopted the culture. Few changed the business model or associated incentive structure.
Where I Part Company with Sachin
This is where my conversation with Sachin begins rather than ends. He asks why leaders tolerate the status quo. I ask why boards reward them for doing so. He emphasizes courage. I emphasize incentives. He sees latent leadership. I see institutional equilibrium. Neither perspective is mutually exclusive. But one operates upstream from the other.
Coming Next
The debate over leadership inevitably leads to a larger historical question. How did American healthcare arrive here? Ironically, many of today’s strategic dilemmas were anticipated nearly forty years ago by one of managed care’s most consequential and controversial architects. Leonard D. Schaeffer believed healthcare organizations would eventually have to stop trying to partner with everyone. Instead, they would have to choose strategic allies capable of building scale together. Whether history vindicated that vision, or exposed its limits, is the subject of Part II.
==##==
Editor’s Note:
For Part II, I’ll trace Leonard Schaeffer’s move from HCFA to Blue Cross of California in 1986, the turnaround, the creation of WellPoint in the early 1990s, and the strategic logic behind selective payer-provider alignment, grounded in contemporaneous sources and Schaeffer’s own writings.
** AI Use & Editorial Standards Disclosure. In producing this content, the author employed AI language tools in a defined supporting role: (1) Research aggregation: surfacing relevant source material and authoritative references across peer-reviewed, institutional, the arts and journalistic databases; (2) Structural organization: proposing content architecture and draft sequencing; (3) Draft suggestion: generating candidate language for author review. The author retains sole editorial responsibility for all published content. Every citation is independently confirmed as accurate and accessible prior to publication. No headlines, pull quotes, or factual claims are published without author verification. AI-generated language is treated as raw material then recast entirely in the author’s established voice and subject-matter expertise before any content reaches publication. This workflow reflects the author’s commitment to the standard that AI serve, not replace the author.

It is cool how a blog I signed up for as my career shifted towards VBC maybe 15 years ago randomly pops back into my inbox with insightful information that is worth reading on a Saturday afternoon as I’m sheltered in an air-conditioned coffee shop.