By Gregg A. Masters, MPH
In the realm of stuff we need to do and sometimes clouded by either ad copy or less than straightforward guru guidance cutting through the clutter can sometimes be confused by the words ‘may’, ‘should’ or other less obligatory statements. For instance:
M/U/S/T | a verb |to:
be commanded or requested to…
be urged to…
be compelled by physical necessity to…
You fill in the blank.
So it’s pretty clear that ‘must’ leaves little wiggle room or cause for doubt when it comes to meeting a certain legal or regulatory threshold or standard. In this case, we’re addressing certain global provisions in the Patient Protection and Affordable Care Act specific to Accountable Care Organizations (ACOs).
CMS previously described ‘patient engagement‘ via the rule making process as:
the active participation of patients and their families in the process of making medical decisions….
[and that] measures for promoting patient engagement may include, but are not limited to, the use of decision support tools and shared decision making methods with which the patient can assess the merits of various treatment options in the context of his or her values and convictions. Patient engagement also includes methods for fostering ‘‘health literacy’’ in patients and their families.
Also consider the balance of criteria or so-called CMS ‘indicia’ of patient centered-ness via Section 425.112: Required processes and patient-centeredness criteria:
“(b) Required processes.
The ACO must define, establish, implement, evaluate, and periodically update processes to accomplish the following:
(2) Promote patient engagement.
These processes must address the following areas:
(i) Compliance with patient experience of care survey requirements in § 425.500.
(ii) Compliance with beneficiary representative requirements in § 425.106.
(iii) A process for evaluating the health needs of the ACO’s population, including consideration of diversity in its patient populations, and a plan to address the needs of its population.
(A) In its plan to address the needs of its population, the ACO must describe how it intends to partner with community stakeholders to improve the health of its population.
(B) An ACO that has a stakeholder organization serving on its governing body will be deemed to have satisfied the requirement to partner with community stakeholders.
(iv) Communication of clinical knowledge/evidence-based medicine to beneficiaries in a way that is understandable to them.
(v) Beneficiary engagement and shared decision-making that takes into account the beneficiaries’ unique needs, preferences, values, and priorities;
(vi) Written standards in place for beneficiary access and communication, and a process in place for beneficiaries to access their medical record.
(3) Develop an infrastructure for its ACO participants and ACO providers/suppliers to internally report on quality and cost metrics that enables the ACO to monitor, provide feedback, and evaluate its ACO participants and ACO provider(s)/supplier(s) performance and to use these results to improve care over time.
(4) Coordinate care across and among primary care physicians, specialists, and acute and post-acute providers and suppliers.
The ACO must—
(i) Define its methods and processes established to coordinate care throughout an episode of care and during its transitions, such as discharge from a hospital or transfer of care from a primary care physician to a specialist (both inside and outside the ACO);”
The pathways to achieve these indicia of patient engagement are perfectly clear, right? Perhaps in the world of mature integrated delivery systems infused with a patient centric mission and committed physician group practice embracing a team based, seamless care culture. But the average ACO tethered to one or more community hospitals via ‘in name only’ cowboy medical groups, I think not.
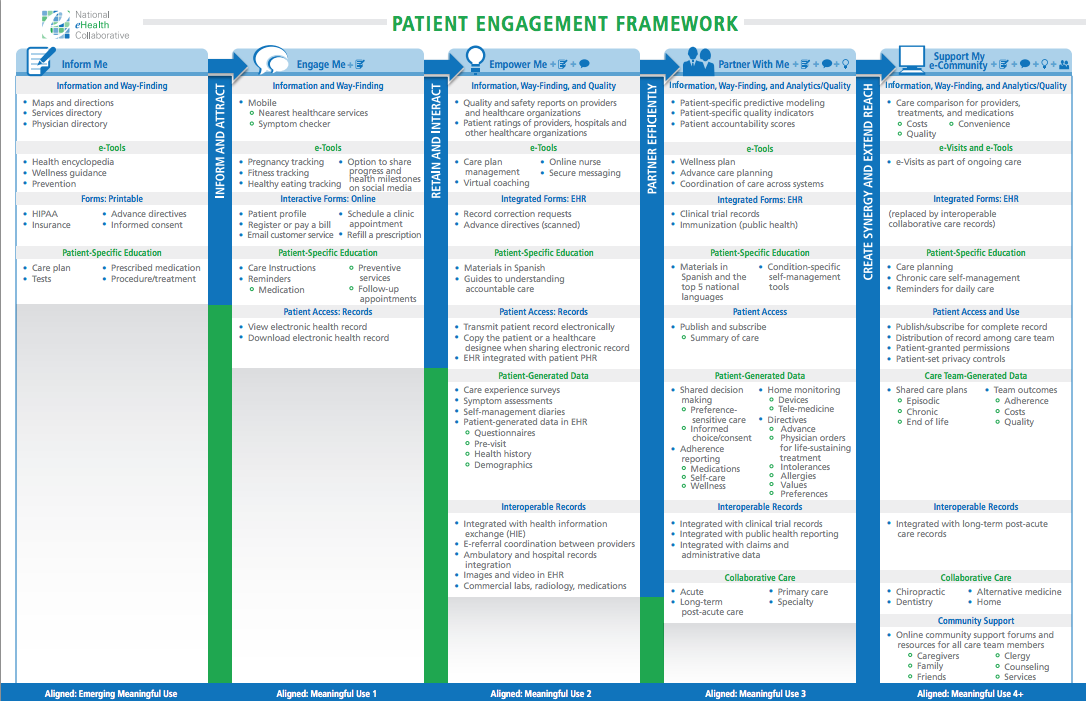
Now consider the crosswalk and ‘best case(?)’ staged implementation timeline perhaps most accurately reflected in the National eHealth Collaborative’s ‘Patient Engagement Framework’.

Truth be told we have a way to go before the proverbial ‘rubber meets the road’, both in terms of the technical fulfillment or health information technology side as well as the ‘fit’ inside an ACO given our national state of ‘readiness’ or maturity if you will.
One bit of news likely to add some clarity to the muddy state of affairs that we’ve learned of recently, and is due to be released shortly by Dave Chase et al at Avado, is a survey of ‘Patient Engagement Readiness’ directed to the ACO industry at large including CEO, CMOs, CIOs, CMIOs and others at the center of this ACO/technology/patient interface. We’ll preview this timely and relevant industry survey and will post the results here as well.
Stay tuned, more to follow shortly!