When Steven Brill published ‘Bitter Pill: Why Medical Bills Are Killing Us‘ in 2013 he brought national attention via a series of personal stories that served to reveal the complex dysfunction inherent in our healthcare delivery and financing system. A veritable ‘conundrum‘ created over the decades of layering managed care complexity (pre-certification, prior authorization, referral management, contract payment adjudication, etc.) on top of the arguably burning ‘fee-for-services’ platform that incentivizes the prevailing ‘do more [units] to earn more [income]’ mentality of hospitals, physicians and allied healthcare practitioners who do not operate in a pre-paid or per member per month capitated environment.
When Steven Brill published ‘Bitter Pill: Why Medical Bills Are Killing Us‘ in 2013 he brought national attention via a series of personal stories that served to reveal the complex dysfunction inherent in our healthcare delivery and financing system. A veritable ‘conundrum‘ created over the decades of layering managed care complexity (pre-certification, prior authorization, referral management, contract payment adjudication, etc.) on top of the arguably burning ‘fee-for-services’ platform that incentivizes the prevailing ‘do more [units] to earn more [income]’ mentality of hospitals, physicians and allied healthcare practitioners who do not operate in a pre-paid or per member per month capitated environment.
Central to Brill’s narrative was the hospital ‘charge master‘, typically a made up fictional schedule of retail (sticker shock) values with ZERO relationship to the actual cost of services provided nor what would ultimately be paid by the patient or third party on his or her behalf.
Brill admonishes readers to:
Pay no attention to the chargemaster – No hospital’s chargemaster prices are consistent with those of any other hospital, nor do they seem to be based on anything objective — like cost — that any hospital executive I spoke with was able to explain. “They were set in cement a long time ago and just keep going up almost automatically,” says one hospital chief financial officer with a shrug.
Most of us are fortunate enough to have 3rd party coverage via our employer or Government funded programs like Medicare, Medicaid, etc., and benefit from deeply discounted intermediary ‘wholesale rates‘ often beginning at 50% of the published charge master rates.
Ironically, those who of us absent this ‘buffer’ and who could least bear the sticker shock burden associated with arbitrary (no relationship to cost) charge master pricing, i.e., the un and under insured, paid the steepest price, see: ‘Medical Bills Are the Biggest Cause of US Bankruptcies: Study‘.
Consumer Directed Health Plans and the ‘Empowered Patient’ Mandate
Since the launch of the Health 2.0 movement and arguably the ‘digital health‘ innovation industry writ large by co-founders Matthew Holt and Indu Subaiya, MD, some of the start-ups launched addressed the problem of price transparency ‘workarounds’ via back end building of ‘virtual’ contract rate books through platform user submissions of EOBs detailing the charge basis and ultimate contract repricing per the health plan negotiated rate of the services rendered and paid. Some of the companies operating in the space, though not necessarily back-ending virtual rate books, include: Medlio, Change Healthcare, Healthcare Bluebook and Castlight Health, see: ‘8 companies working on healthcare price transparency‘.
Clearly the ‘holy grail‘ here is contract rate-book transparency, but don’t hold your breath. These rates are deemed proprietary and thus closely guarded ‘trade secrets’.
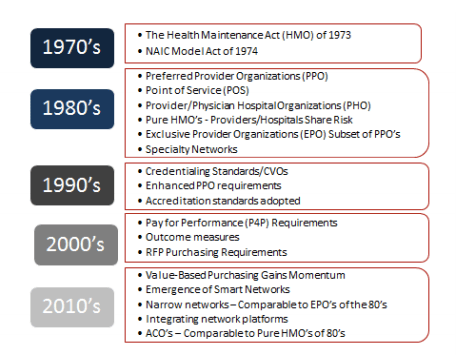
So fast forward to today. It’s 2016 (some 43 years post HMO Act) and healthcare inflation which has shown remarkable restraint principally due to the lingering impact of the great recession of 2008, coupled with the health insurance industry’s new found love affair fueled by the ACA with so called ‘consumer directed health plans‘ (aka code for the ‘cost shifting’ charade). Think of it this way, massive health plans, pooling millions of lives, extracting maximum pricing leverage from providers and exercising varying degrees of medical management oversight have explicitly admitted that as an industry they can NOT manage clinical risk, thus have chosen make provider pricing restraint ‘our’ problem. Afterall, they reasoned the required (mythical absence of?) ‘skin in the game‘ of high deductibles, non-covered services, copayments and co-insurance drives granular price sensitivity since the once 3rd party buffer (if it ever existed) is no longer present to immunize our exposure to the cost of utilizing healthcare services.
Last month The Health Care Incentives Improvement Institute (HCI3 ) and Catalyst for Payment Reform (CPR) issued the fourth installment of the ‘Report Card on State Price Transparency Laws‘. The picture below tells the less than pretty story:

They open the report noting:
Despite the full integration of price information into almost every other retail experience, it’s typical in American health care for consumers to go into an appointment or procedure knowing nothing about what it will cost until long afterward
And conclude as follows:
Our 2016 Report Card on State Price Transparency Laws shows that price transparency—an obvious expectation integrated into every other consumer experience—is on the minds of state legislators and other health care leaders throughout the U.S. It also highlights why this information is so critical to every health care consumer in every state; prices for routine and very common procedures can vary by more than 50 percent, even in the same geographical area, placing a potentially significant financial burden on individual consumers, a burden that can be avoided with robust health care price transparency. Thus, design and implementation of the legislation matter.
In fact, the potential for transparency to empower consumers, shift costs down, and raise quality rests entirely on the strength and comprehensiveness of each state law’s implementation. This is a perspective that is often lost in some of the research on the effectiveness of price transparency, even though no one should be surprised that weak resources yield poor results. Importantly, a very strong and thorough body of research demonstrates that consumers will seek lower-priced, high-quality providers when given the right information in the right format.
Many states may see low grades for themselves. However, in this report card, they also have a roadmap for improvement. It’s up to states to apply that roadmap to benefit from the desired and proven positive effects of price and quality transparency.
I am not as optimistic as the authors that price transparency solutions coupled with a growing army of ‘empowered patients‘ are sufficient to tame the rapacious appetite of a predominantly volume incentivized delivery system. Clearly this is a slog unlike any other industry re-tooling, re-invention or re-engineering challenge we’ve EVER faced in the United States. More will be revealed as we move from niche solutions (concierge medicine, direct practice, non-risk bearing ACOs or IDNs, or HMO-lite solutions, etc.) tweaking at the margins of the ecosystem dysfunction but delivering little by way of sustainable contribution.
As I was recently reminded by Dan Munro of a quote often mis-attributed to Winston Churchill:
The question is whether there is any reason to believe that such a new era [think value based healthcare driven by ’empowered patients’] may yet come to pass. If I am sanguine on this point, it is because of a conviction that men and nations do behave wisely once they have exhausted all other alternatives. Surely the other alternatives of war and belligerency [avoiding the inevitable path of risk assumption/integration] have now been exhausted. Abba Eban, June 1967
Bottom-line?
I see HMO’s 2.0 (global risk) in our future. There just isn’t anyway around it, though we’re trying our best to avoid the inevitable.
Your thoughts?